The most common cause of heel pain is plantar fasciitis. It is usually caused by a biomechanical imbalance resulting in tension along the plantar fascia. The diagnosis is typically based on the history and the finding of localized tenderness. Treatment consists of medial arch support, anti-inflammatory medications, ice massage and stretching. Corticosteroid injections and casting may also be tried. Surgical fasciotomy should be reserved for use in patients in whom conservative measures have failed despite correction of biomechanical abnormalities. Heel pain may also have a neurologic, traumatic or systemic origin.
Plantar fasciitis, the most common cause of heel pain, may have several different clinical presentations. Although pain may occur along the entire course of the plantar fascia, it is usually limited to the inferior medial aspect of the calcaneus, at the medial process of the calcaneal tubercle. This bony prominence serves as the point of origin of the anatomic central band of the plantar fascia and the abductor hallucis, flexor digitorum brevis and abductor digiti minimi muscles.
Plantar fasciitis is often referred to as “heel spur syndrome” in the literature and the medical community, but the label is a misnomer. This vague and nonspecific term incorrectly suggests that osseous “spurs” (inferior calcaneal exostoses) are the cause of pain rather than an incidental radiographic finding. There is no correlation between pain and the presence or absence of exostoses,1 and excision of a spur is not part of the usual surgery for plantar fasciitis.2 Plantar fasciitis occurs in both men and women, but is more common in the latter. Its incidence and severity correlate strongly with obesity.
Etiology
Most cases of plantar fasciitis are the result of a biomechanical fault that causes abnormal pronation. For example, a patient with a flexible rearfoot varus may at first appear to have a normal foot structure but, on weight-bearing, may display significant pronation. The talus will plantar flex and adduct as the patient stands, while the calcaneus everts. This pronation significantly increases tension on the plantar fascia.
Other conditions, such as tibia vara, ankle equinus, rearfoot varus, forefoot varus, compensated forefoot valgus and limb length inequality, can cause an abnormal pronatory force. Increased pronation with a collapse produces additional stress on the anatomic central band of the plantar fascia and may ultimately lead to plantar fasciitis.2,3 This is understandable since the weakest point of the plantar fascia is its origin, not its substance (because of the high tensile strength of the fascial fibers themselves).4
Presenting Symptoms
Patients usually describe pain in the heel on taking the first several steps in the morning, with the symptoms lessening as walking continues. They frequently relate that the pain is localized to an area that the examiner identifies as the medial calcaneal tubercle. The pain is usually insidious, with no history of acute trauma. Many patients state that they believe the condition to be the result of a stone bruise or a recent increase in daily activity. It is not unusual for a patient to endure the symptoms and try to relieve them with home remedies for many years before seeking medical treatment.
Diagnosis
Even in this age of modern technology, the diagnosis of plantar fasciitis is based mainly on the medical history and clinical presentation. Direct palpation of the medial calcaneal tubercle often causes severe pain (Figure 1). The pain is generally localized at the origin of the anatomic central band of the plantar fascia, with no significant pain on compression of the calcaneus from a medial to a lateral direction. Standard weight-bearing radiographs in the lateral and anteroposterior projection demonstrate the biomechanical character of the hindfoot and forefoot, and may show other osseous abnormalities such as fractures, tumors or rheumatoid arthritis in the calcaneus. However, radiographs usually serve only as an aid to confirm the clinician's diagnosis.
FIGURE 1.

Palpation of the medial calcaneal tubercle usually elicits pain in patients presenting with plantar fasciitis.
Conservative Treatment
Conservative treatment of plantar fasciitis should address the inflammatory component that causes the discomfort and the biomechanical factors that produce the disorder. Patient education is imperative. Patients must understand the etiology of their pain, including the biomechanical factors that caused their symptoms. They should learn about home therapy that may relieve some discomfort and about recommended changes in daily activities, such as wearing appropriate athletic shoes with a significant medial arch while walking. Patients whose symptoms are associated with a recent increase in exercise should adopt a less strenuous regimen until the plantar fasciitis resolves.
The patient is fitted with a removable longitudinal metatarsal pad during the first visit. This pad, which is created from felt, 1/4-in thick, extends from the distal aspect of the medial calcaneal tubercle to about 0.5 cm proximal to the five metatarsal heads. The clinician should skive (cut or bevel) this pad so that its greatest thickness is under the medial aspect of the arch, as opposed to the lateral aspect of the foot. This pad serves as a temporary medial arch support to decrease pronation during midstance of the gait cycle.
Other clinicians favor placing a medial arch pad directly against the patient's skin and taping the patient's foot from a plantar medial to a plantar lateral direction using 3-in wide tape. These temporary devices provide greater biomechanical support than over-the-counter heel cups or heel pads. If a patient has significant plantar fasciitis pain secondary to a limb-length inequality or unilateral ankle equinus, a simple 1/4-in heel lift in the shoe of the affected foot may provide temporary relief.
Stretching the Achilles tendon is beneficial as adjunctive therapy for plantar fasciitis. The patient is instructed to face a wall with one foot approximately 6 in from the wall and the other foot about 2 ft from the wall, and then lean toward the wall while keeping both heels on the floor. This exercise stretches the heel cord of the limb that is farther from the wall. It should be performed with both legs forward for two minutes each, three to five times daily. This stretching program should be continued for six to eight weeks, after which time the patient is reevaluated.
Each night for 10 to 14 days, the patient should apply an ice pack to the plantar aspect of the heel 15 to 20 minutes before going to bed. An alternative approach is to massage the plantar fascia with an ice block (made up of water frozen in a paper cup) for 15 minutes per day for two weeks.
It is often advantageous for patients with no contraindication to take a nonsteroidal anti-inflammatory drug (NSAID) for six to eight weeks. We believe that corticosteroid injections should be avoided in the initial treatment of plantar fasciitis; we use them only as supplemental treatment in patients who have resistant chronic plantar fasciitis after achieving adequate biomechanical control. These injections may provide only temporary relief and can cause a loss of the plantar fat pad if used injudiciously. Typically, 3.0 mL of an equal mixture of 1 percent lidocaine, 0.5 percent marcaine and 1 mL of triamcinolone (40 mg per mL) is injected around the medial process of the calcaneal tuberosity. Solutions containing epinephrine are not used. Radiographic guidance of injection placement may aid the inexperienced practitioner.
Night splints that maintain the foot at an angle of 90 degrees or more to the ankle have recently been used as adjunctive therapy for plantar fasciitis. These orthoses prevent contraction of the plantar fascia while the patient sleeps. One study5 showed relief of recalcitrant plantar fasciitis pain in 83 percent of patients treated with such splints.
Orthotic devices are the mainstay of ongoing conservative treatment for patients with plantar fasciitis. The biomechanical factors that cause the abnormal pronatory forces stressing the medial band of the plantar fascia must be corrected. Patients with pes cavus feet may benefit from using a flexible orthotic device with an additional heel cushion. This prescription orthosis can disperse some of the force experienced on heel strike, while maintaining biomechanical support for propulsion. Prescription orthoses provide long-term relief by reducing abnormal stress on the plantar fascia.
The clinician should perform a complete biomechanical examination, checking the range of motion of the first metatarsophalangeal, midtarsal, subtalar and ankle joints, as well as the forefoot-to-rearfoot relationship, to adequately correct for any biomechanical abnormalities. To make the orthosis, the clinician should cast the foot with the subtalar joint in the neutral position, neither inverted nor everted. Casting performed in this position captures the foot deformity and allows for proper biomechanical control. A properly casted orthosis will provide biomechanical support and diminish the abnormal compensatory force that may subsequently cause plantar heel pain. Family physicians who do not elect to learn and utilize the skills necessary to provide this type of care may refer patients to podiatrists or orthopedic surgeons with an interest in such treatment.
Some clinicians advocate the use of a short-leg walking cast for several weeks as a final conservative step in the treatment of plantar fasciitis. In one study,6 a short-leg cast worn for a minimum of three weeks was found to be an effective form of treatment for chronic plantar heel pain.
Surgical Management
Adequate conservative therapy of plantar fasciitis, as described above, must be pursued for several months before any surgical intervention is contemplated. It is unwise to operate on a patient who has had only a limited trial of conservative treatment and who has incomplete control of the abnormal mechanics that have caused the symptoms. Surgical intervention may be indicated in the small percentage of patients who have failed to benefit from conservative methods and who still have significant plantar heel pain after a lengthy period of treatment.
It is well documented that plantar fasciotomy alone, without inferior calcaneal exostectomy, is an effective surgical approach to this condition5,6 (Figure 2). Endoscopic plantar fasciotomy was developed as a minimally invasive way of accomplishing this.5–7 Endoscopic plantar fasciotomy is less traumatic than traditional open heel-spur surgery and allows earlier weight-bearing after surgery. Some authorities consider the technique controversial, but a study8 of 652 endoscopic plantar fasciotomy procedures, performed by 25 different surgeons, reported a success rate (resolution of chronic plantar fasciitis) as high as 97 percent. Results of a recent study9 that compared 29 endoscopic procedures with 84 open fasciotomies with spur resection indicate that patients who underwent endoscopic plantar fasciotomy returned to work an average of 55 days sooner than those who had an open heel approach (29 days versus 84 days). Depending on their job, patients may return to work as soon as the next day. Those whose work involves standing or walking or is otherwise physically demanding may need up to eight weeks of partial weight-bearing.
FIGURE 2.
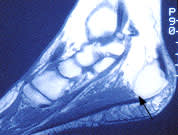
Sagittal magnetic resonance image of fat pad, showing the complexities of the fibrous septal network, the plantar fascia and an inferior calcaneal exostosis (arrow) just superior to the plantar fascia.
Other Causes of Heel Pain
Less common causes of heel pain should be considered before a treatment regimen for plantar fasciitis is undertaken. These include sciatica, tarsal tunnel syndrome, entrapment of the lateral plantar nerve, rupture of the plantar fascia, calcaneal stress fracture and calcaneal apophysitis (Sever's disease). Rarely, systemic disorders can cause heel pain.
Sciatica
Heel pain secondary to sciatica is a result of pressure on the L5-S1 nerve root, which provides segmental innervation to the posterior thigh, and the gluteal, anterior, posterior and lateral leg muscles, as well as sensation to the heel. This nerve root is also responsible for the plantar response (ankle reflex). The sciatic nerve innervates numerous muscles along its course, and patients may experience weakness in any or all of them. They may also report sharp pain radiating down the buttocks and the posterior aspect of the thigh and leg distally toward the heel.
The patient's lower extremities should be evaluated while the patient sits on the examination table with knees flexed. The neurologic examination should include testing of proprioception, sharp/dull sensation and reflexes (specifically the plantar reflex) to rule out polyneuropathy, sciatica and neuralgia as causes of the heel pain. The physical examination should also include the simple thigh and leg raise, which, if painful, may indicate a disorder of the lower back. The treatment of heel pain caused by sciatic root compression should be directed toward the primary pathology.
Tarsal Tunnel Syndrome
Tarsal tunnel syndrome is caused by compression of the posterior tibial nerve as it courses from the posterior aspect of the medial malleolus toward the anteromedial aspect of the calcaneus. The tarsal canal is a fibro-osseous structure bounded by the flexor retinaculum medially, the posterior aspect of the talus and calcaneus laterally, and the medial malleolus anteriorly. The tendons of the posterior tibialis, the flexor digitorum longus and the flexor hallucis longus muscles, as well as the posterior tibial nerve, artery and vein, course within this space. Compression of the posterior tibial nerve here may cause a burning sensation.
Specific conditions that may cause compression of the posterior tibial nerve include a soft tissue mass, callus from a previous fracture of the medial malleolus, inflammation of one of the tendons coursing through the tarsal canal and excessive pronation that increases tension on the posterior tibial tendon and the corresponding nerve. Patients may describe heel pain with a tingling sensation around the plantar and medial aspect of the heel. Symptoms are often exacerbated by weight-bearing and ambulation but may persist at rest.
The posterior tibial nerve is responsible for a large area of sensory innervation, and patients often experience difficulty in pinpointing their discomfort to a specific location in the heel. Unlike patients with heel pain from plantar fasciitis, those with tarsal tunnel syndrome typically describe their pain as being most intense on standing and walking after long periods of rest. They usually do not experience pinpoint tenderness at the origin of the medial band of the plantar fascia.
Physical examination should include palpation of the course of the posterior tibial nerve from the proximal aspect of the medial malleolus distally toward the anterior aspect of the calcaneus. Patients may experience an uncomfortable burning pain that radiates proximally toward the calf (Valleix sign) or distally toward the toes (Tinel's sign).
Finally, the clinician should inspect the patient's hindfoot for any structural conditions that may alter the patient's biomechanics. An abnormal gait can create greater tension on the contents of the posterior tarsal tunnel, resulting in an irritation of the posterior tibial nerve.
Nerve conduction velocity studies and electromyographic tests can confirm the diagnosis of tarsal tunnel syndrome. Conservative therapy should address excessive pronation, which can cause compression of the posterior tibial nerve. Reduction of ambulation, NSAIDs, physical therapy and orthotic devices may alleviate these symptoms. Patients who do not respond sufficiently to conservative therapy may require surgical decompression of the tarsal canal.
Entrapment of the Lateral Plantar Nerve
Entrapment of the first branch of the lateral plantar nerve, which provides innervation to the abductor digiti quinti muscle, has been said to cause plantar medial heel pain. The entrapment usually occurs between the abductor hallucis muscle and the quadratus plantae muscle, giving patients a burning sensation on the plantar aspect of the heel that is aggravated by daily activities and may even persist at rest. Palpation of this area may prove painful, with a tingling sensation. The same conservative modalities that are used to treat plantar fasciitis are effective in treating this condition.
Plantar Fascial Rupture
Rupture of the plantar fascia is an uncommon cause of plantar heel pain. Patients often report severe pain in the medial arch following physical trauma. Some patients have been misdiagnosed and treated unsuccessfully for several months with steroid injections for presumed plantar fasciitis. Magnetic resonance imaging can aid greatly in the diagnosis of this condition.
Physical examination may reveal a palpable deficit in the plantar fascia or a small enlarged area at the distal aspect of the plantar fascial rupture. Patients also experience severe pain on palpation of the plantar fascia, with maximal tenderness generally distal to the medial process of the calcaneal tuberosity. Gait analysis usually reveals a significant limp that spares the affected limb. Treatment consists of immobilization with a nonweight-bearing short-leg cast or a removable boot cast and a regimen of NSAID therapy. Immobilization for four to six weeks is usually required before ambulation without pain is possible.
Calcaneal Stress Fracture
Acute heel pain caused by calcaneal stress fractures can closely resemble the symptoms usually associated with plantar fasciitis. The history may reveal a recent abrupt increase in daily exercise or other activities. Patients with this condition often report increased pain on direct medial to lateral compression of the calcaneus (Figure 3). This type of elicited pain is rarely present in patients with plantar fasciitis.
FIGURE 3.

Medial to lateral compression of the calcaneus typically causes pain in patients with calcaneal stress fracture.
Conservative therapy involves educating patients to limit activities that make the pain worse. Patients are advised to wear athletic shoes all day (they diminish the forces of heel strike) and are instructed to moderate their activities for three weeks. If the symptoms are not relieved significantly in three weeks, the patient is reevaluated, and the foot is placed in a removable cast boot.
Calcaneal Apophysitis
Calcaneal apophysitis (Sever's disease) usually affects boys between six and 10 years of age, chiefly those who are obese and those who are extremely active. In most cases, the pain is located in the posterior aspect of the calcaneus and is more severe after athletic activity.
Palpation of the posterior aspect of the calcaneus around the insertion of the Achilles tendon usually reveals local tenderness. Patients with this disorder may have a tight Achilles tendon with limited ankle dorsiflexion, which sometimes causes patients to walk on their toes to decrease the pain.
The treatment is usually simple. All strenuous, high-impact activities are discontinued during the initial phase of treatment, and heel lifts, ice massage and appropriate NSAID therapy are prescribed. This regimen is followed (as soon as inflammation is decreased to a point that stretching is not painful) by stretching exercises to achieve adequate dorsiflexion of the ankle joint. Orthotic devices can be prescribed after the acute inflammation has resolved to reduce the probability of recurrence. Cast immobilization is occasionally necessary in patients whose symptoms do not resolve in a timely manner and in noncompliant children.
Systemic Disorders
Heel pain may occur in patients with various systemic inflammatory conditions, including rheumatoid arthritis, ankylosing spondylitis, psoriatic arthritis, Reiter's syndrome, gout, Behçet's syndrome and systemic lupus erythematosus.10–18 Gonorrhea and tuberculosis have also been implicated as causes of heel pain, but such an association is rare.19
Most patients with systemic disease present with joint pain and inflammation in other areas of the body, but symptoms may occasionally begin in the heel. A detailed history and physical examination may disclose the symptom complexes of an arthritic disease. For example, a young man who reports bilateral heel pain and who has a history of conjunctivitis or urethritis for more than one month may have Reiter's disease. Similarly, heel pain in a patient with a history of psoriasis and asymmetric pain in the distal inter-phalangeal joints of the fingers and toes should raise the possibility of psoriatic arthritis. When heel pain is of systemic origin, treatment should, of course, be directed at the primary disease state. Radiographs of patients with systemic inflammatory conditions may show posterior or plantar exostoses, but these findings are not clinically important.
The number of patients whose heel pain is caused by systemic arthritic diseases is small in comparison to those with pain from other causes, but these arthritic diseases must be ruled out through appropriate physical examination and laboratory studies before the heel pain is treated.
