
A more recent article on common finger fractures and dislocations is available.
Am Fam Physician. 2012;85(8):805-810
Related letter: Proper Technique for Reduction of Metacarpophalangeal Dislocations
Author disclosure: No relevant financial affiliations to disclose.
Finger fractures and dislocations are common injuries that are often managed by family physicians. A systematic physical examination is imperative to avoid complications and poor outcomes following these injuries. Radiography (commonly anteroposterior, true lateral, and oblique views) is required in the evaluation of finger fractures and dislocations. Dorsal dislocation of the proximal interphalangeal joint is the most common type of finger dislocation. Finger dislocations should be reduced as quickly as possible and concurrent soft tissue injuries treated appropriately. Referral to a hand specialist is needed if a dislocation cannot be reduced; is unstable following reduction; or involves significant ligament, tendon, or soft tissue injury. Some common finger fractures can be treated conservatively with appropriate reduction and immobilization. Referral to a hand specialist is required if a fracture is unstable, involves a large portion (greater than 30 percent) of the intra-articular surface, or has significant rotation.
Finger fractures and dislocations may occur during daily activities, such as work, but usually occur during participation in sporting activities. Finger and metacarpal fractures are the most common sports-related fractures in adults and adolescents.1,2 If not treated properly, finger fractures and dislocations can have significant consequences, including poor function, chronic pain, stiffness, and deformity.3 The goal of management is return to normal function and activity. Appropriate referral to a hand surgeon may prevent delay in necessary treatment. Table 1 summarizes the evaluation and management of finger dislocations and fractures.
| Clinical recommendation | Evidence rating | References |
|---|---|---|
| Finger fractures involving greater than 30 percent of the intra-articular surface should be referred to an orthopedic or hand surgeon. | C | 9, 16, 17 |
| Following reduction of a proximal interphalangeal dislocation, short-term splinting in flexion with early active range of motion and strengthening is preferable to prolonged immobilization. | B | 5, 10 |
| Treatment of a mallet fracture includes splinting the distal interphalangeal joint in extension; various splint types are of equal benefit. | B | 13–15 |
| Displaced, oblique, or spiral finger fractures should be referred to a hand surgeon. | C | 3 |
| Diagnosis | Examination and initial treatment | Management | Recommendations for referral |
|---|---|---|---|
| PIP dislocation |
|
| Fractures involving greater than 30 to 40 percent of the intra-articular surface, reduction is difficult or unsuccessful, the patient is unable to obtain full extension following reduction |
| MCP dislocation (especially in the thumb) |
|
| Reductions requiring anesthesia, open reductions |
| DIP dislocation |
|
| Complicated injuries |
| Distal phalanx fracture (tuft fracture) |
|
| Rarely needed |
| Mallet fracture |
|
| Conservative treatment is ineffective; large displaced bony fragment or significant volar subluxation |
| Flexor digitorum profundus avulsion fracture |
|
| All injuries |
| Middle or proximal phalanx fracture |
|
| Displaced, oblique, or spiral fractures |
General Approach to Finger Injuries
ASSESSMENT
The history should include mechanism of injury, timing and progression of symptoms, hand dominance, and any previous finger injury. A physical examination is crucial in the assessment of finger injuries. Common signs of injury are local swelling, erythema, pain, deformity, and tenderness to palpation. The assessment should also include finger alignment, ligament integrity, neurovascular status, and flexion and extension of the joints. Assessment of stability is necessary for appropriate management of dislocated joints.
A systematic approach to the finger examination avoids missed diagnoses, potential complications, and poor outcomes. Radiographic evaluation with a minimum of three views (commonly anteroposterior, true lateral, and oblique) is required if any fracture or dislocation is suspected.4
MANAGEMENT
Management of finger injuries begins with closed reduction of the fracture or dislocation, if indicated. Stability of the reduction is assessed by gentle active flexion of the involved finger; the joint should be stable through flexion and extension. Rotation is assessed after a finger fracture by active flexion; there should be no digital overlap. All fingernail beds should point toward the thenar eminence. Stabilization is often achieved with splinting. Postreduction radiography can be used to assess alignment. If there is instability or significant rotation, referral to a hand surgeon is required.
Dislocations
Finger dislocations can occur at the distal interphalangeal (DIP), proximal interphalangeal (PIP), or metacarpophalangeal (MCP) joints. The PIP joint is the most commonly dislocated finger joint.5 Injuries to the MCP joint often occur in the thumbs.6 Dislocations of DIP joints are commonly traumatic and often complicated by fracture and soft tissue injury.7
PIP JOINT
The PIP joints are primarily stabilized by the matching articular phalangeal surfaces plus supportive soft tissue structures, including the collateral ligaments and volar plates. Dislocations are described as dorsal, volar, or lateral depending on the direction of the middle phalanx to the proximal phalanx.
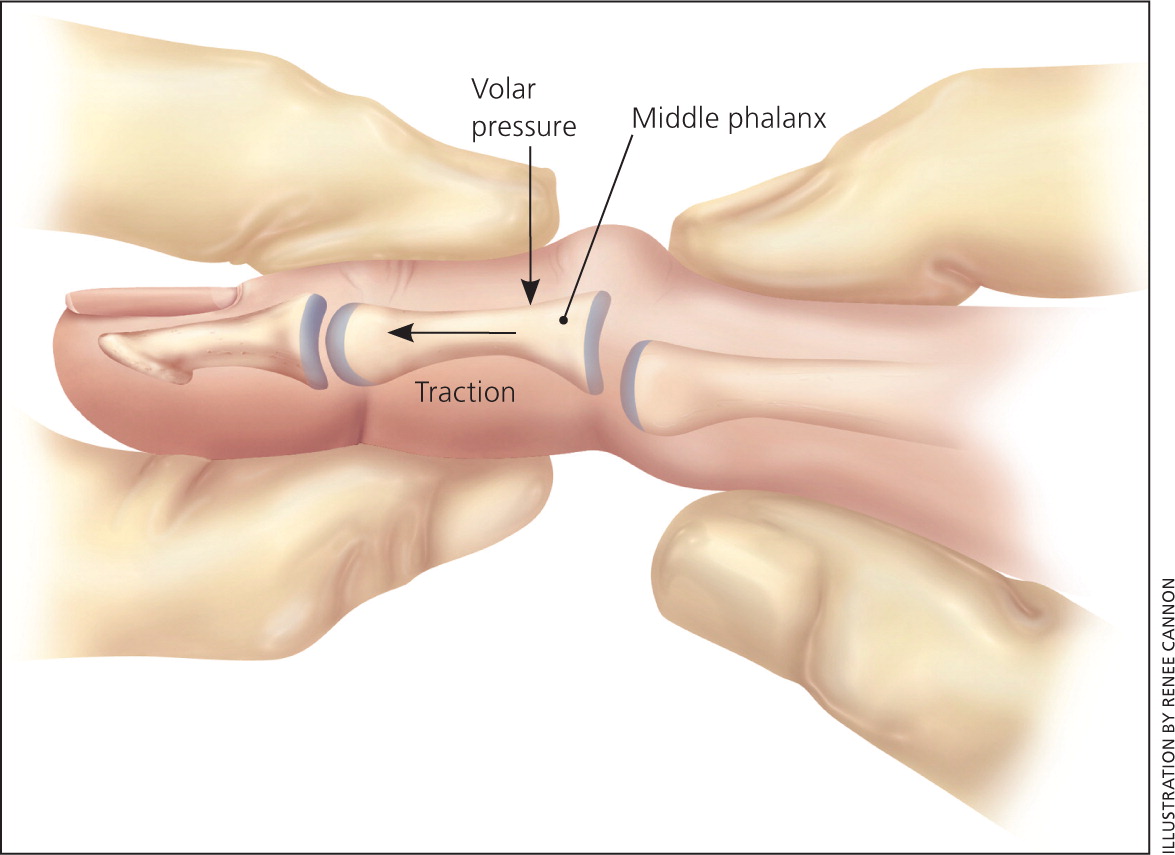
A dorsal PIP dislocation is the most common type of finger dislocation. It usually involves injury to the volar plate and may include a volar plate avulsion fracture. A dorsal PIP dislocation often leads to obvious dorsal deformity of the middle phalanx and volar plate tenderness. If relocation of the joint is unsuccessful or if the joint remains unstable following reduction and subsequently dislocates again, the injured finger should be evaluated using radiography. Radiography also helps identify volar fracture of the middle phalanx and other associated injuries.
Reduction of a dorsal PIP dislocation should be attempted at the time of injury, if possible, by applying traction and volar pressure on the middle phalanx at the PIP joint (Figure 1). Successful relocation produces immediate relief of discomfort and resolution of the deformity. Reduction is often successful without anesthesia. A local joint block can be considered if significant pain impedes reduction. The possibility of concomitant fracture or soft tissue injury must be considered, especially if relocation is unsuccessful. Radiography should be performed before further reduction attempts.
Radiography is also required following successful reduction to evaluate for subluxation, instability of the PIP joint, and possible volar plate fractures of the middle phalanx. Volar plate fractures may be small and can be treated conservatively. The risk of subluxation and instability is higher with larger volar plate fractures.8 Referral to a hand specialist is indicated if more than 30 percent of the volar intra-articular surface is involved, or if subluxation or instability of the PIP joint is detected.9 Flexion and extension at the PIP joint should be evaluated following successful reduction of a dislocation. If extensive loss of motion persists, referral is recommended. Failure to treat PIP dislocations appropriately can lead to chronic pain, degenerative changes, and loss of function.
Traditional treatment following reduction of uncomplicated dorsal PIP joint dislocations is splinting for one to two weeks followed by buddy taping for another one to two weeks. The benefits of early range of motion following relocation of a dorsal PIP dislocation are debated. A study showed an increase in range of motion and intrinsic muscle strength following four weeks of splinting with daily active exercise compared with immobilization alone.10 For uncomplicated dorsal PIP dislocations, short-term splinting in flexion with early active range of motion and strengthening is preferable to immobilization.5,10
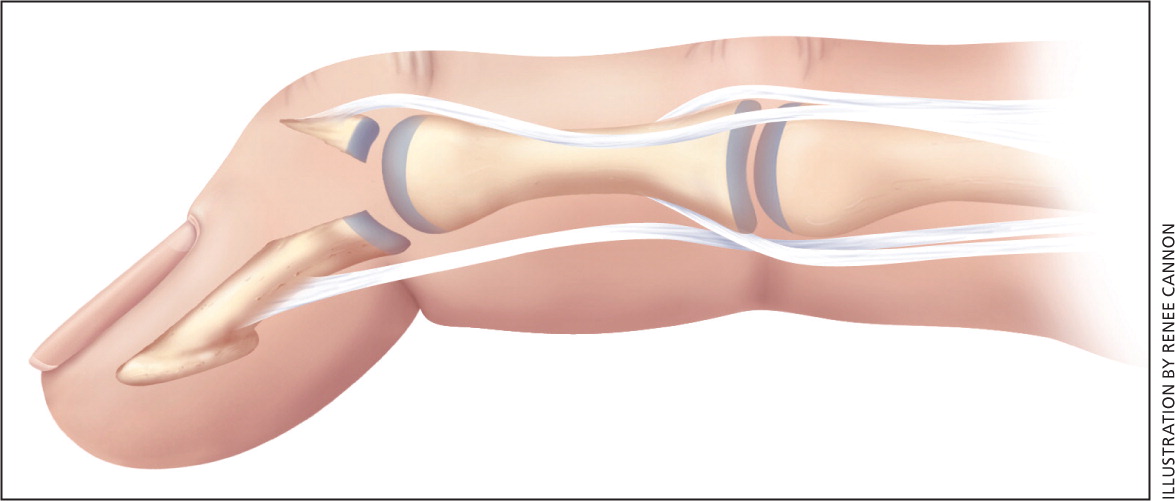
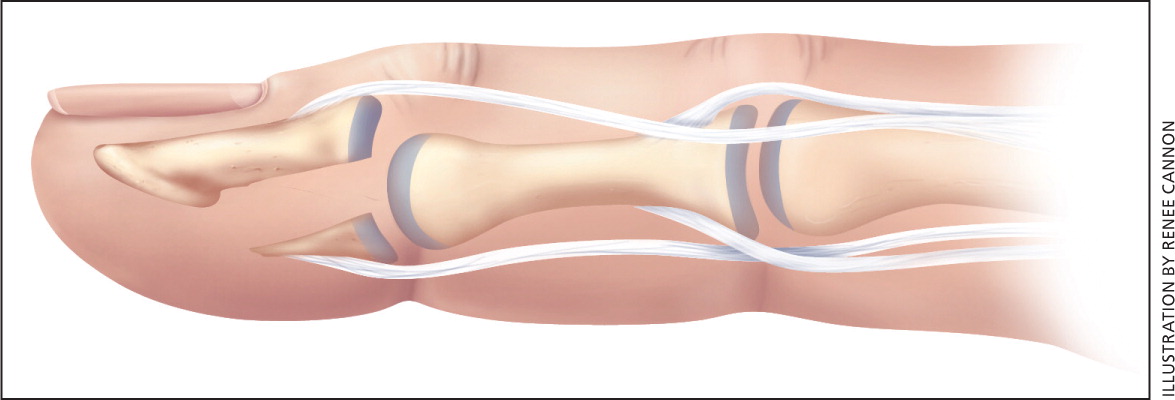
Lateral and volar PIP dislocations are less common than dorsal injuries. A volar dislocation (Figure 2) can be accompanied by avulsion of the central slip extensor mechanism of the PIP. Central slip injury can lead to the inability to extend the finger at the PIP joint and hyperflexion or boutonnière deformity over time.11 These injuries should be splinted for six weeks in full PIP extension to avoid chronic deformity at the PIP joint.11 Volar PIP dislocations are more difficult to reduce and results should be confirmed with postreduction radiography. Referral is recommended for fracture involving greater than 30 to 40 percent of the intra-articular surface, if reduction is difficult or unsuccessful, or if the patient is unable to achieve full extension following reduction.

MCP JOINT
Dislocations of the MCP joint are usually dorsal.6 Simple dislocations do not involve soft tissue structures and are reduced using the same technique as with dorsal PIP dislocations. Reduction may be unsuccessful because of soft tissue injury or fracture. Radiography and referral are recommended for reduction requiring anesthesia and for open reductions.7 Following a simple MCP reduction, radiography is needed to assess congruity of the joint. Treatment consists of splinting in slight flexion with early range of motion and strengthening exercises.
DIP JOINT
Dislocations of the DIP joint are often associated with trauma and may have associated fractures and soft tissue injury.7 A simple dorsal DIP dislocation should be evaluated with radiography to assess for fracture. Reduction is similar to that of a dorsal PIP dislocation if no concomitant injury is present. Treatment following simple reduction is also similar to that following PIP dislocation. Referral is recommended for complicated injuries.
Fractures
Several types of fractures can involve the phalanx or the intra-articular surface. Failure to identify and appropriately treat these fractures can lead to long-term reduced function and disability.
DISTAL PHALANX FRACTURES
Tuft fracture (Figure 3) is the most common type of distal phalanx fracture. This fracture at the fingertip is often associated with a crush injury. Distal phalanx fractures are stable and can be treated with simple splinting of the DIP joint only. Splinting for two to four weeks should be followed by range of motion and strengthening of the DIP joint. Any soft tissue and nail bed injuries associated with these fractures must be recognized and treated. Patients should be informed that these fractures are often complicated by hyperesthesia, pain, and numbness for up to six months following the injury.12

MALLET FRACTURES
Mallet fractures (mallet finger) occur at the insertion of the terminal finger extensor mechanism into the dorsal portion of the distal phalanx. These fractures are caused by an axial load to the tip of an extended finger, leading to forced flexion at the DIP joint.11 A mallet fracture includes a bone fragment attached to the terminal extensor mechanism (Figure 4).
Treatment of a mallet fracture includes splinting the DIP joint in extension for eight weeks. It is imperative that extension is maintained at all times during treatment because any flexion can affect healing and may extend the treatment period. Radiography must be performed following splint application to confirm congruity of the fracture fragment with the distal phalanx in the joint space.3 Studies show no difference in outcomes among splint types as long as DIP extension is maintained.13–15
Referral for surgical management of mallet fractures has been suggested for those involving greater than 30 percent of the intra-articular surface and for those associated with volar subluxation of the distal phalanx.16,17 Nevertheless, a study of 22 mallet fractures involving greater than 30 percent of the joint space reported that patients with volar subluxation and displaced fragments after splinting had no difference in pain and function than those without these features.18 Conservative therapy for all mallet fractures is preferable as first-line treatment and may have outcomes similar to those of surgical treatment.19,20 Consultation with a hand surgeon is recommended if the physician is uncomfortable with the management of more complicated mallet fractures.
FLEXOR DIGITORUM PROFUNDUS AVULSION FRACTURE
The flexor digitorum profundus tendon inserts at the volar surface of the distal phalanx. An avulsion fracture (Figure 5) typically results from forced hyperextension of a flexed DIP joint. This injury is commonly referred to as jersey finger.11 Examination of the affected finger demonstrates the inability to flex the finger at the DIP joint. Because of the risk of tendon retraction and the need for surgical treatment, patients with flexor digitorum profundus avulsion fractures should be referred to a hand specialist.
MIDDLE AND PROXIMAL PHALANX FRACTURES
Middle and proximal phalanx fractures are often associated with trauma. These injuries should be suspected with gross deformity on inspection of the middle or proximal phalanx. These fractures are commonly classified as intra- or extra-articular. Intra-articular fractures are often complicated and unstable and should be referred to a hand specialist.3 Extra-articular fractures may be nondisplaced or displaced. Stable nondisplaced fractures can be treated conservatively with buddy taping and early range of motion, but should be followed carefully to ensure stability of the fracture. Displaced, oblique, or spiral fractures are inherently unstable and should be referred to a hand specialist.3
