Fatigue is among the top 10 reasons patients visit primary care offices, and it significantly affects patients' well-being and occupational safety. A comprehensive history and cardiopulmonary, neurologic, and skin examinations help guide the workup and diagnosis. Fatigue can be classified as physiologic, secondary, or chronic. Physiologic fatigue can be addressed by proper sleep hygiene, a healthy diet, and balancing energy expenditure. Secondary fatigue is improved by treating the underlying condition. Cognitive behavior therapy, exercise therapy, and acupuncture may help with some of the fatigue associated with chronic conditions. Myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS) is a chronic, severe, and potentially debilitating disorder with demonstrated inflammatory, neurologic, immunologic, and metabolic abnormalities. ME/CFS has a poor prognosis, with no proven treatment or cure. It may become more common after the COVID-19 pandemic because many patients with long COVID (post–COVID-19 condition) have symptoms similar to ME/CFS. The most important symptom of ME/CFS is postexertional malaise. The 2015 National Academy of Medicine diagnostic criteria diagnose ME/CFS. Exercise can be harmful to patients with ME/CFS because it can trigger postexertional malaise. Patients should be educated about pacing their activity not to exceed their limited energy capacity. Treatment should prioritize comorbidities and symptoms based on severity.
Fatigue is one of the top 10 reasons for a visit to primary care and is reported by 5% to 10% of patients in the primary care setting.1,2 Fatigue is the most common symptom reported by those with chronic illness.3 A cross-sectional survey found up to 38% of U.S. workers reported fatigue during the previous two weeks.4 Fatigue is strongly associated with absenteeism, decreased work productivity, and serious accidents.5,6 Fatigue is estimated to cost employers more than $100 billion per year.4 Risk factors for fatigue in the general population include being female, unmarried, younger, and of lower educational attainment.7 Fatigue is an important component of frailty syndrome, which is commonly found in older patients with limited physiologic reserves and vulnerability to minor illness or injury, and independently predicts falls and functional decline in older people.8–10 Decreased cognition, some forms of cancer, metabolic and reproductive health effects, and increased mortality have been associated with fatigue.9,11
SORT: KEY RECOMMENDATIONS FOR PRACTICE
| Clinical recommendation | Evidence rating | Comments |
|---|---|---|
| Evaluate for physiologic causes of fatigue before investigating secondary or chronic fatigue.15,16,19 | C | Expert opinion and consensus guidelines |
| Use exercise therapy and psychological interventions (particularly cognitive behavior therapy) to treat fatigue related to cancer, inflammatory conditions, neurologic conditions, and fibromyalgia, but not ME/CFS.15,16,19,26–33,36,51,52 | B | Limited-quality patient-oriented evidence |
| Use the National Academy of Medicine criteria to diagnose ME/CFS.19,38 | C | Consensus guideline informed by systematic review |
| When treating ME/CFS, target the most severe symptoms and comorbidities.15,16,19,51,52 | C | Expert opinion and consensus guidelines |
| Educate patients with ME/CFS about pacing, which may prevent postexertional malaise.15,16,19 | C | Expert opinion and consensus guidelines |
ME/CFS = myalgic encephalomyelitis/chronic fatigue syndrome.
A = consistent, good-quality patient-oriented evidence; B = inconsistent or limited-quality patient-oriented evidence; C = consensus, disease-oriented evidence, usual practice, expert opinion, or case series. For information about the SORT evidence rating system, go to https://www.aafp.org/afpsort.
BEST PRACTICES IN OCCUPATIONAL MEDICINE
| Recommendation | Sponsoring organization |
|---|---|
| Do not routinely order sleep studies (polysomnography) to screen for or diagnose sleep disorders in workers having chronic fatigue or insomnia. | American College of Occupational and Environmental Medicine |
Source: For more information on Choosing Wisely, see https://www.choosingwisely.org. For supporting citations and to search Choosing Wisely recommendations relevant to primary care, see https://www.aafp.org/pubs/afp/collections/choosing-wisely.html.
Fatigue encompasses a range of potential causes and related comorbidities and is a feeling of weariness or exhaustion.12 This can be a physiologic, self-limited, normal response in healthy individuals. It may also be chronic or secondary to another condition. Fatigue may or may not respond to rest. In comparison, sleepiness is the tendency to doze off and responds to rest.13 Patients, physicians, and medical journals use the words fatigue, sleepiness, and weakness interchangeably; the three are often related and not mutually exclusive. There are widely used objective and subjective tools to assess and monitor sleepiness.13 In contrast, assessment tools for fatigue are not consistently validated and tend to be condition specific.14
Evaluation
The differential diagnosis list for fatigue is extensive (Table 1).15,16 Table 2 provides a list of questions to ask when eliciting a history from a patient with fatigue.16 Physicians should use validated screening tools to rule out comorbid sleep, mood, and substance use disorders. Figure 1 suggests an approach to evaluating patients with fatigue. Medications should be reviewed to ensure the fatigue is not iatrogenic. A physical including cardiopulmonary, neurologic, and skin examinations should be performed. The initial laboratory workup should be guided by history, physical examination, and common causes of fatigue. Laboratory testing without specific indications is not high-yield and may only change treatment in 5% of patients.17
TABLE 1. Diseases and Conditions Associated With Fatigue and Options for Evaluation
| Category | Disease/conditions | Evaluation options |
|---|---|---|
| Cardiovascular and pulmonary | Arrhythmias Cardiomyopathy Chronic obstructive pulmonary disease Coronary artery disease Heart failure Pulmonary hypertension Sarcoidosis Valvular heart disease | Chest computed tomography Chest radiography Echocardiography Electrocardiography Holter monitor Pulmonary function testing |
| Endocrine and metabolic | Chronic kidney disease Diabetes mellitus Hypercalcemia Hypercortisolism Hyperthyroidism Hypothyroidism Primary adrenal insufficiency Severe obesity | A1C level Adrenocorticotropic hormone level Basic metabolic panel Cortisol level Renal ultrasonography Thyroid-stimulating hormone level Thyroid ultrasonography Urinalysis |
| Environmental and exposure-related | Adverse medication effect Gulf War syndrome Heavy metals Mold/mycotoxins Substance use disorder | Alcohol screening (e.g., SBIRT [screening, brief intervention, and referral to treatment]) Chest radiography Lead level Medication levels Urine drug screening |
| Gastrointestinal | Celiac disease Cirrhosis Food allergy or intolerances* Inflammatory bowel diseases Small intestinal bacterial overgrowth* | Abdominal computed tomography Comprehensive metabolic panel C-reactive protein Endomysial antibody Erythrocyte sedimentation rate Liver ultrasonography Tissue transglutaminase |
| Gynecologic | Endometriosis Pregnancy Premenstrual syndrome | Pelvic ultrasonography Urine pregnancy test |
| Hematologic | Anemia Iron overload | Complete blood count Ferritin level Folate level Iron panel Vitamin B12 level |
| Infectious diseases | Coccidioidomycosis COVID-19 Epstein-Barr virus* Giardiasis Hepatitis B Hepatitis C HIV Parvovirus B19 Q fever Syphilis Tick-borne diseases Tuberculosis West Nile virus | Epstein-Barr virus antibody Hepatitis B antigen Hepatitis C antibody HIV testing Lyme titer Monospot Purified protein derivative or quantiferon Rapid plasma reagin Serum treponemal antibody Stool ova and parasites |
| Neurologic | Cerebrospinal fluid leak Cerebrovascular accident Chiari malformation Craniocervical instability Multiple sclerosis Myasthenia gravis Parkinson disease Seizures Spinal stenosis Traumatic brain injury Vitamin B12 deficiency | Acetylcholine receptor antibody Brain or spine magnetic resonance imaging Electroencephalography Methylmalonic acid level Vitamin B12 level |
| Oncologic | Primary cancers Secondary cancers | Bone scan Complete blood count with differential Positron emission tomography/computed tomography |
| Primary psychiatric | Anxiety* Bipolar disorder Depression* | Generalized Anxiety Disorder 7-item screening tool Medication levels Mood Disorder Questionnaire Patient Health Questionnaire-9 Thyroid-stimulating hormone level |
| Rheumatologic | Fibromyalgia* Polymyalgia rheumatica Polymyositis Rheumatoid arthritis Systemic lupus erythematosus | Anti-cyclic citrullinated peptides antibody Antinuclear antibodies C-reactive protein Creatine phosphokinase Erythrocyte sedimentation rate Radiography of affected joints Rheumatoid factor |
| Sleep | Narcolepsy Periodic limb movement disorder* Sleep apnea* | Epworth Sleepiness Scale Polysomnography STOP-Bang (snoring, tired, observed, pressure, body mass index, age, neck size, gender) questionnaire |
*—Comorbid conditions commonly found with myalgic encephalomyelitis/chronic fatigue syndrome.
TABLE 2. Questions for Eliciting a History From a Patient With Fatigue
| History Typical reaction to activity that was previously tolerated? Any preceding triggers to the start of fatigue? Duration of symptoms? Pattern of symptoms? Function How would you rate your level of fatigue? What helps relieve your fatigue? What exacerbates your fatigue? In what level of function can you participate? How does it compare with before you became sick? How does your illness affect your ability to work and manage household responsibilities? How do you feel when you try to “push through” the fatigue? Postexertional malaise How do you feel after normal physical or emotional activity? How much activity does it take you to feel ill? What symptoms do you experience when standing or exerting yourself? How much time is required for recovery from physical or mental exertion? What activity avoidance or modification do you have to make due to your illness? | Sleep-related Do you have any trouble falling asleep or staying asleep? After sleeping, do you feel rested? How would you describe your sleep quality? Do you require more naps than other people? Cognition-related Do you have problems performing the following activities? Driving Watching a movie Reading Completing timed complex tasks Following/participating in conversation Doing more than one thing at a time Compare your work/school success before and after becoming ill. Orthostasis Describe how you feel when you have been standing still for more than a few minutes. What happens when you quickly change position from lying down or sitting to standing? How long can you tolerate standing before feeling sick? How does hot weather affect you? Do you study or work in a reclined position? Why? |
Adapted with permission from Bateman L, Bested AC, Bonilla HF, et al. Myalgic encephalomyelitis/chronic fatigue syndrome: essentials of diagnosis and management. Mayo Clin Proc. 2021;96(11):2868.
FIGURE 1.
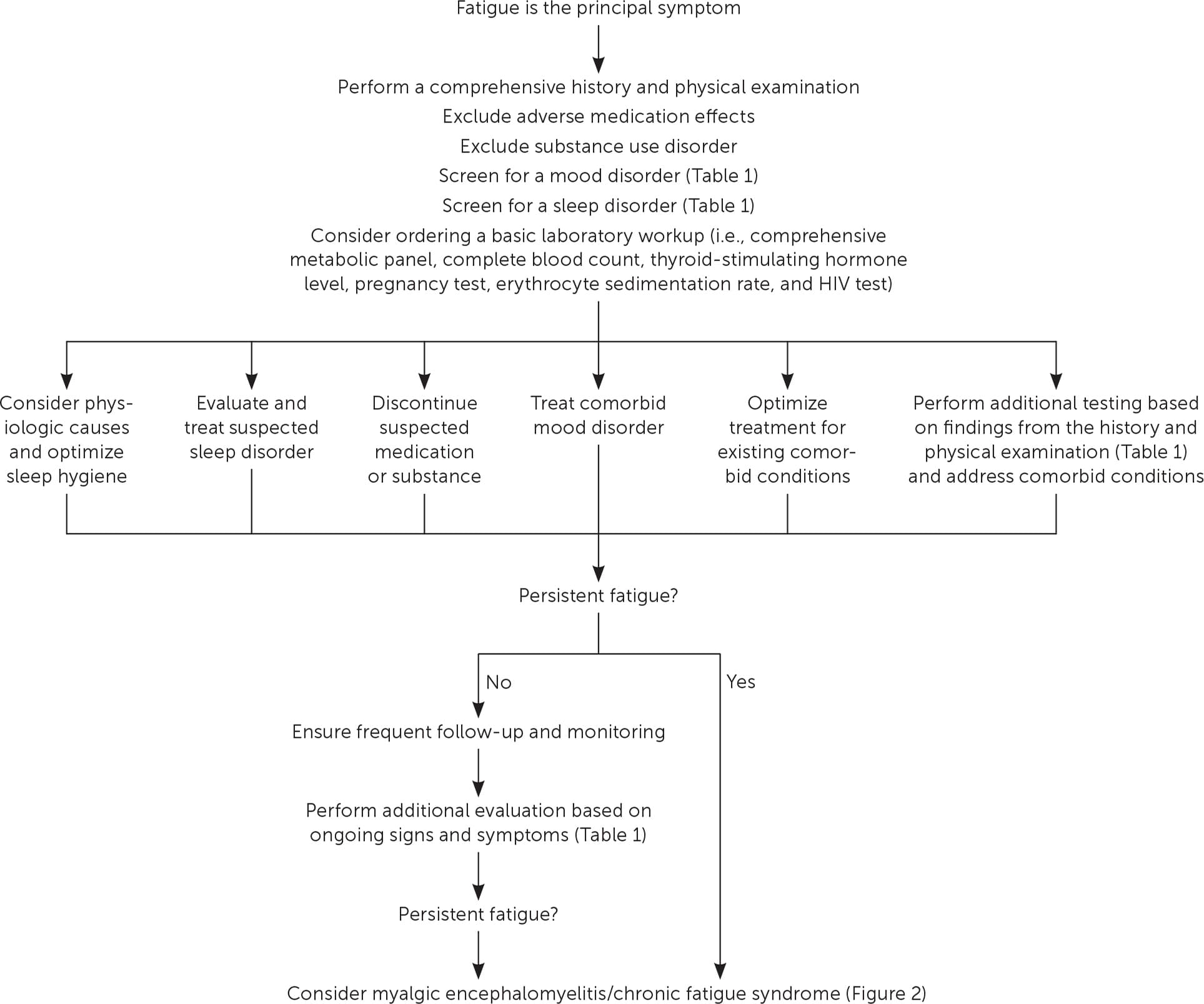
Suggested approach for evaluating fatigue in primary care.
Despite a comprehensive workup, a definitive diagnosis is often not made. In one study investigating first-time reports of fatigue in young adults without known comorbid conditions presenting to primary care, most received a workup; however, only 27% were diagnosed with a condition that could explain the fatigue, the most common of which included anemia, vitamin B12 deficiency, infection, pregnancy, and psychiatric diagnoses.17 In another study, only 8% of patients received a clear condition-based diagnosis one year after their presentation to primary care with fatigue. Nearly 17% received a psychological diagnosis.18
Physiologic Fatigue
Physiologic fatigue, caused by an imbalance between activities that burn energy and those that restore energy, is a normal response relieved by appropriate rest. Physiologic causes of fatigue should be assessed before investigating secondary or chronic fatigue.15,16,19 Physicians should inquire about the patient's daily habits, including the amount and quality of sleep, activity level throughout the day, and nutritional status. Inadequate sleep is a widespread problem, with nearly 30% of U.S. adults reporting fewer than seven hours of sleep per night.20 Patients at high risk of obstructive sleep apnea should be screened using a validated tool such as the STOP-Bang (snoring, tiredness, observed apnea, blood pressure, body mass index, age, neck circumference, gender) questionnaire.21 Good sleep hygiene can contribute to more restorative sleep. Patients should be reminded to adhere to consistent sleep schedules, limit screen time, and avoid caffeine and alcohol near bedtime.22 Excessive exercise of prolonged intensity and duration that depletes energy stores and does not allow for adequate recovery can leave patients feeling fatigued.23 A prerequisite to having the energy to perform daily tasks is consuming the nutritional components to create this energy. Physicians should ask patients about their dietary habits and counsel them to avoid fad diets or excessively restrictive meal regimens. Ginseng may be helpful with nonspecific physiologic fatigue.24
Secondary Fatigue
Fatigue is a common symptom of many disorders. Treatment should target the underlying condition. For example, pulmonary rehabilitation helps the respiratory symptoms of chronic obstructive pulmonary disease and also fatigue.25 Exercise therapy and psychological interventions, specifically cognitive behavior therapy, have some evidence of effectiveness in fatigue related to cancer,26 inflammatory conditions (e.g., rheumatoid arthritis, inflammatory bowel disease),27,28 and neurologic conditions (e.g., multiple sclerosis, myasthenia gravis).29,30 Exercise may improve fatigue and function related to fibromyalgia.31,32 Tai chi may be superior to aerobic exercise for those with fibromyalgia.33 Massage and acupuncture may help manage cancer-related fatigue.34,35 There is no evidence that pharmacologic treatment targeting fatigue (e.g., modafinil, methylphenidate) helps manage fatigue related to most chronic diseases.36,37
Chronic Fatigue
Fatigue lasting six months or longer is considered chronic. Many common diseases are associated with chronic fatigue.15 Most people with protracted fatigue do not have chronic fatigue syndrome.18 However, when a patient has fatigue for six months or longer, and physiologic and secondary causes are excluded, physicians should consider a diagnosis of myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS).
Myalgic Encephalomyelitis/Chronic Fatigue Syndrome
ME/CFS is a chronic, complex, multisystem, incompletely understood, and variably defined condition with a poor prognosis.15 In 2015, the National Academy of Medicine renamed the condition and published recommendations with evidence-based diagnostic criteria16,19,38 (Table 316,19 ). The diagnostic criteria have been widely adopted; however, the name systemic exertional intolerance disease is not commonly used.15,16
TABLE 3. National Academy of Medicine Criteria for Diagnosing Myalgic Encephalomyelitis/Chronic Fatigue Syndrome
| Required core symptoms (present for at least six months, at least 50% of the time, with moderate to severe intensity): |
| Postexertional malaise (i.e., crash or postexertional symptom exacerbation) |
| Profound fatigue of new onset with substantially decreased ability to engage in pre-illness levels of activity or function |
| Unrefreshing sleep |
| Plus, at least one of the following: |
| Cognitive impairment (i.e., brain fog) |
| Orthostatic intolerance (e.g., lightheadedness, nausea, fatigue, palpitations, syncope with prolonged standing) |
| Other common clues and associated symptoms (not part of the criteria): |
| Gastrointestinal or genitourinary symptoms |
| Hypersensitivity to external stimuli (e.g., light, noise, chemicals, foods, drugs) |
| Impaired immune function and increased susceptibility to infection |
| Influenza-like symptoms (e.g., sore throat, lymphadenopathy, chills, fever) |
| Onset after an infectious episode (e.g., mononucleosis, COVID-19) |
| Respiratory issues (e.g., air hunger) |
| Thermoregulatory issues |
| Visual disturbances |
| Widespread pain |
Adapted with permission from Committee on the Diagnostic Criteria for Myalgic Encephalomyelitis/Chronic Fatigue Syndrome; Board on the Health of Select Populations; Institute of Medicine. Beyond Myalgic Encephalomyelitis/Chronic Fatigue Syndrome. Redefining an Illness. National Academies Press; 2015:210, with additional information from reference 16.
DIAGNOSIS
An ME/CFS diagnosis requires the patient to experience severe fatigue that produces a substantial decrease from pre-illness function. The secondary fatigue associated with most chronic diseases improves with exercise. In contrast, patients with ME/CFS can experience a prolonged worsening of symptoms with even a small increase in a previously tolerated activity. This is called postexertional malaise15,16 (Table 415,19 ). Patients refer to it as a crash or relapse. Postexertional malaise can be provoked by physical exertion but also by challenges in the emotional, cognitive, and sensory realms. The symptoms of postexertional malaise are far more severe than expected from simple overexertion by a patient who is not physically fit. Postexertional malaise is the most important feature of ME/CFS and distinguishes it from other fatigue-causing conditions.
TABLE 4. Characteristics of Postexertional Malaise
| Provoked by challenges in any of the following areas: Cognitive Emotional Environmental Orthostatic Physical Sensory | Symptoms Exacerbation of any constellation of symptoms (e.g., cognitive, pain, sleep, influenza-like) Individual limits somewhat predictable; can vary from day to day Severity out of proportion to stimulus Worsening function compared with baseline | Timing Immediately following trigger or may be delayed by hours or days May last days, weeks, or months after provoking incident Patient may never return to baseline |
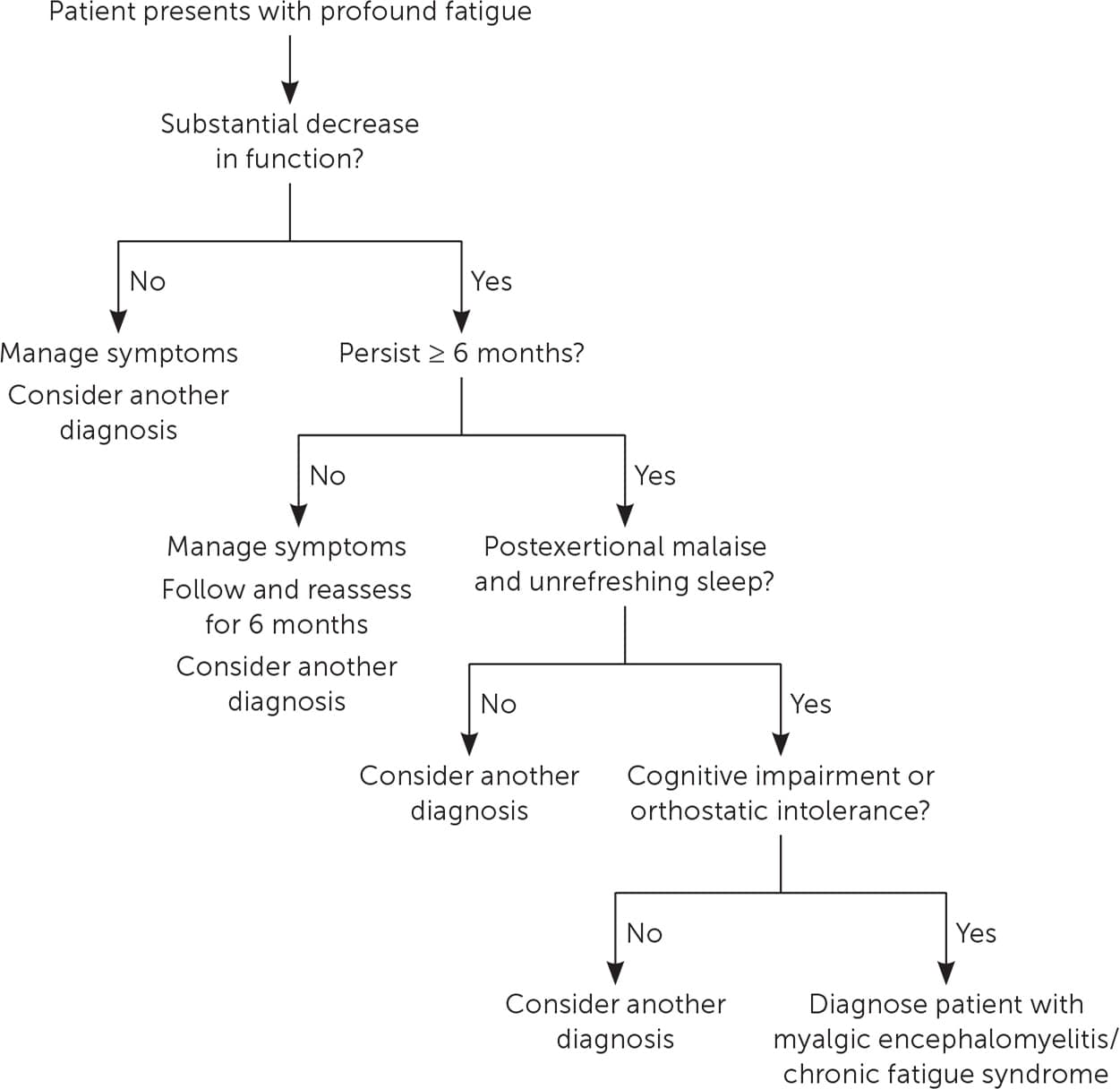
There are no physical examination findings or diagnostic tests for ME/CFS. It was previously a diagnosis of exclusion but now is a clinical diagnosis16,39 (Figure 219 ). ME/CFS is not a psychological disorder and is not caused by physical deconditioning, laziness, or malingering. Patients with this disorder have debilitating symptoms and frequently face stigma and skepticism from friends, family, and physicians. 40 Patients often know more about ME/CFS than their physicians, and many have little trust in the medical establishment.41
FIGURE 2. Diagnosis of myalgic encephalomyelitis/chronic fatigue syndrome.
Adapted with permission from Committee on the Diagnostic Criteria for Myalgic Encephalomyelitis/Chronic Fatigue Syndrome; Board on the Health of Select Populations; Institute of Medicine. Beyond Myalgic Encephalomyelitis/Chronic Fatigue Syndrome. Redefining an Illness. National Academies Press; 2015:212.
ME/CFS may be difficult to diagnose due to an extensive differential, variable clinical presentations, multiple possible comorbid conditions, and a lack of medical education and awareness among physicians42 (Table 115,16 ). Any condition associated with chronic fatigue, chronic pain, autonomic dysfunction, or immune dysregulation can overlap with ME/CFS and cloud the clinical picture.
EPIDEMIOLOGY
ME/CFS may affect 0.8% to 2.2% of the U.S. population, but most are undiagnosed or misdiagnosed.43 The COVID-19 pandemic may increase the prevalence because many patients with long COVID (post–COVID-19 condition) report long-lasting sequelae, including chronic fatigue.44 Women are affected three to four times more often than men.43 Most patients are White, but prevalence data are lacking in people of color.15 The patient's age at diagnosis is bimodal, with a peak in the teenage years and another peak in the thirties, but the condition has been described in people from two to 77 years of age.16
Patients with ME/CFS and their family members report worse function and quality of life scores than patients with other severe chronic diseases such as multiple sclerosis.45,46 The severity of illness varies, with 25% of patients able to work. Between 10% and 25% are homebound or bedbound.47 The most severely affected patients often cannot access medical care and are usually not included in studies of ME/CFS. Other patients have waxing and waning symptoms and functional status.47
PATHOPHYSIOLOGY
Researchers have found abnormalities in energy metabolism in the nervous and immune systems in patients with ME/CFS.15,48 Patients exhibit impaired generation and utilization of adenosine triphosphate, the key energy-storing molecule in aerobic metabolism.49 When patients underwent maximal exercise over two consecutive days, the patients with ME/CFS demonstrated significantly impaired exercise performance on day 2 compared with healthy participants and even patients with multiple sclerosis.50
MEDICAL CARE
There is no U.S. Food and Drug Administration–approved treatment for ME/CFS.51 The most valuable action a physician can take for a patient with this disorder is to validate their concerns.15,16 A healthy patient-physician relationship is only possible when the patient feels believed. The physician should treat symptoms in order of severity, with the patient setting the priority 19 (Table 515,16,51–53 ). The goal of treatment should be to minimize symptoms and maximize function, which may include facilitating access to resources available to any severely disabled patient.___ANCHOR_START___/afp20230700p58-sort4___ANCHOR_END___ Physicians should treat any comorbidities and educate patients about pacing, where the patient stays within their finite energy capacity to avoid triggering postexertional malaise. Patients can use the mantra “Stop, rest, pace.”15,16,19,54,55 Helpful pacing resources can be found at https://www.meaction.net/resource/pacing-and-management-guide.54 The Centers for Disease Control and Prevention website provides patient-centered handouts at https://www.cdc.gov/me-cfs/resources/patient-toolkit.html.55
TABLE 5. Treatment Options for Symptoms of Myalgic Encephalomyelitis/Chronic Fatigue Syndrome
| Symptom | Nonpharmacologic treatments | Pharmacologic treatments (start at low doses) |
|---|---|---|
| Fatigue or brain fog | Cognitive pacing Memory aids (e.g., calendar reminders, alarms, calculator) Perform cognitive tasks lying down | Occasional use; beware of “push and crash”: Amantadine Armodafinil (Nuvigil) Caffeine Methylphenidate Modafinil |
| Gastrointestinal | Healthy diet Trial of elimination diets (e.g., aspartame, sugar, dairy, gluten-free) | If small intestinal bacterial overgrowth: Metronidazole (Flagyl) Oral vancomycin Rifaximin (Xifaxan) |
| Hypersensitivity to stimuli | Environmental controls to reduce light levels, sound levels, and temperature fluctuations | None |
| Immune dysfunction | Avoid crowds Frequent hand washing Mask in public | Selective use: Antiviral agents (e.g., acyclovir) Hydroxychloroquine Intravenous immunoglobulin Subcutaneous gamma globulin |
| Orthostatic intolerance | Avoidance of prolonged standing Compression stockings Electrolyte drinks Salt tablets | Alpha agonists Desmopressin Fludrocortisone Intravenous saline Low-dose beta blocker |
| Pain | Acupuncture Chiropractic therapy Dry needling Heat or cold packs Hydrotherapy Massage Pacing Physical therapy Transcutaneous electrical nerve stimulation | Antiepileptics Medical marijuana Muscle relaxers Naltrexone (Revia) Nonsteroidal anti-inflammatory drugs Serotonin and norepinephrine reuptake inhibitors Tramadol |
| Postexertional malaise | Assistive devices (e.g., scooter, shower chair, stair lift) Avoid triggers Disability benefits Handicap parking placard Home health aide Pacing Use symptom journal or activity tracker to learn limits Work or school accommodations | None |
| Sleep problems | Blue-light filter Ear plugs Eye masks Good sleep hygiene Light therapy Meditation and relaxation techniques | Alpha blockers Antiepileptics Antihistamines Benzodiazepines Eszopiclone (Lunesta) Low-dose tricyclic antidepressants Mirtazapine Muscle relaxers Suvorexant (Belsomra) Trazodone Zolpidem |
Note: Treatment should be individualized, symptom-based, and prioritized by the patient.
Treatment must be individualized because every patient with ME/CFS has different symptoms. Polypharmacy can become a problem, so using medications with more than one therapeutic effect is helpful (e.g., prescribing a tricyclic antidepressant to help with both poor sleep and pain). Frequent medication reconciliation is imperative. Patients may be sensitive to adverse medication effects; therefore, lower doses to start should be considered and increased slowly as indicated.
Regularly scheduled visits foster the patient-physician partnership and help continually reassess and optimize symptom-directed therapy. Physicians should offer telemedicine visits because even an outing to a physician's office may trigger postexertional malaise. Because many of these patients are homebound, telemedicine can help them access much-needed care. Specialists should be consulted as needed and could include psychology, pain medicine, physiatry, occupational therapy, physiotherapy, and sleep medicine.52
OUTDATED RECOMMENDATIONS AND CONTROVERSY
In 2011, the PACE trial reported that graded exercise therapy and cognitive behavior therapy were effective treatments for patients with ME/CFS.56 The study was later found to have significant methodologic flaws and investigator-related conflicts of interest.57 Reanalyzed data showed no benefit of interventions and showed harms in the graded exercise therapy group.58 Importantly, exercise is no longer recommended by the U.S. ME/CFS Clinician Coalition and is likely to be harmful compared with standard care.15,16,59 Cognitive behavior therapy may be as helpful as it would be for anyone with a chronic debilitating disease, but it does not help with fatigue.
This article updates previous articles on this topic by Yancey and Thomas,60 Rosenthal, et al.,61 and Craig and Kakumanu.62
Data Sources: A search was completed in PubMed using the key terms fatigue, sleepiness, screening for obstructive sleep apnea, myalgic encephalomyelitis/ chronic fatigue syndrome. Additional terms included prevalence, diagnosis, treatment, prognosis, definition, measurement, cost, and productivity. Essential Evidence Plus and the Cochrane database were also searched in addition to reference lists in retrieved articles. Priority included articles published since 2012 and focused on meta-analyses, systematic reviews, specialty society guidelines, and randomized controlled trials. Search dates: June 2022, July 2022, November 2022, and April 2023.
