
A more recent article on childhood eye examinations is available.
Am Fam Physician. 2001;64(4):623-629
Early and accurate detection of eye disorders in children can present a challenge for family physicians. Visual acuity screening, preferably performed before four years of age, is essential for diagnosing amblyopia. Cover testing may disclose small-angle or intermittent strabismus. Leukocoria, which is detected with an ophthalmoscope, may indicate retinoblastoma or cataract. Children with glaucoma may have light sensitivity and enlargement of the cornea, and conjunctivitis that does not respond quickly to treatment may reflect more serious ocular inflammation. Children with serious eye injuries often present to the primary care physician. Nystagmus and many systemic conditions are associated with specific eye findings.
Some eye disorders in children must be diagnosed at an early age to prevent loss of vision and to optimize treatment outcomes.1–4 Unfortunately, effective screening for eye disorders and visual function can be difficult for primary care physicians. Young children may not be willing participants in the screening process, and interesting fixation devices are often not available in the office. In addition, some of the diagnoses are complex. The involvement of pediatric ophthalmologists with specialized training, expertise and examination equipment is often required.
Despite these difficulties, most significant eye problems in children can be identified with effective screening techniques. The American Academy of Family Physicians, the American Academy of Pediatrics and the American Association for Pediatric Ophthalmology and Strabismus have endorsed the role of the primary care physician in screening children for eye disorders.5 If possible, all children should have their monocular visual acuity tested before four years of age.
The purpose of this article is to facilitate recognition and referral of children with significant eye disorders, emphasizing eight conditions that are easily missed during visits to the primary care office. These conditions are amblyopia, small-angle strabismus, leukocoria, glaucoma, ocular inflammation, eye trauma, nystagmus and systemic disorders that affect the eye.
Amblyopia
Amblyopia (lazy eye) is defined as a reduction in best-corrected visual acuity that is not directly attributable to any structural abnormality of the eye or visual pathway. With a prevalence of 2 percent,6 it is the most common cause of uncorrectable loss of vision in children. The visual outcome can range from 20/25, or nearly normal, to worse than 20/200, or legally blind. With effective detection and early treatment, most vision loss associated with this condition can be avoided.
Most cases of amblyopia affect only one eye, but some cases are bilateral. Ophthalmologists refer to anisometropic amblyopia when one eye is involved and isometropic amblyopia when the condition is bilateral. Although the first few years are the most crucial, amblyopia may occur in children as old as four to six years. There are three major categories of amblyopia, each with special problems for diagnosis and treatment.7
STRABISMIC AMBLYOPIA
Strabismic amblyopia is the most common type of amblyopia. The deviating eye which may turn in (esotropia), out (exotropia), up (hypertropia) or down (hypotropia), is suppressed in order to prevent double vision. This suppression can become so effective that the affected eye loses its visual potential. The diagnosis becomes difficult when the deviation is small and thus is not obvious.
REFRACTIVE AMBLYOPIA
Refractive amblyopia is the most difficult type of amblyopia to detect. If the two eyes have significantly different refractive states, the young child may rely on the sight of the more focused eye, causing the other eye to lose its visual potential. The child will appear to see normally at home and in the primary care office because the normal eye is being used for visual tasks. If both eyes are out of focus, both may become amblyopic.
DEPRIVATION AMBLYOPIA
Deprivation amblyopia is the most severe type in terms of loss of vision. It typically affects children with unilateral or bilateral congenital cataracts but also may occur in those with corneal or vitreous opacity, severe ptosis (droopy eyelid) or excessive patching. Deprivation amblyopia develops because the retina does not receive a clear image. In some cases, the cataract may not be apparent on casual penlight inspection but is detected by the absence or distortion of red reflex on ophthalmoscopic examination.
TREATMENT
Treatment of amblyopia begins with appropriate optical correction using eyeglasses or contact lenses. In the absence of strabismus, this passive treatment may be effective after several months. The classic therapy is occlusion or patching of the normal eye. Nearly full-time occlusion is often prescribed initially. Follow-up evaluations are recommended at intervals that vary depending on the age of the child, and are more frequent for younger children. Recently, “penalization” with atropine to blur the dominant eye has been increasingly used as an alternative to patching.
Treatment is always most effective if started early. Children with suspected strabismus, even if mild or intermittent, should be referred for evaluation beginning around four to six months of age. An infant with a constant large-angle esotropia can be referred even earlier. Eyelid hemangiomas or other masses, even if subtle, can cause changes in refraction and may result in refractive amblyopia; children with these problems should be referred as early as possible. The ophthalmoscope should be used to examine the red reflex beginning in the neonatal period, and children with suspected media opacities should be referred urgently. Children with a family history of amblyopia are at increased risk, and the importance of early vision screening cannot be overemphasized.
Small-Angle Strabismus
Although many cases of strabismus are obvious, others may be difficult to detect because the deviations are small or intermittent. Accommodative esotropia, which usually begins in toddlers who are farsighted, is an example. Because of their eyes' refractive state, these children are forced to accommodate excessively and induce accommodative convergence, normally part of the near reflex, even when looking at distant objects. Treatment with eyeglasses, including bifocals in some cases, may help to align the eyes. Unfortunately, small-angle esotropia is at least as likely as more significant deviations to be associated with amblyopia.8 Cover testing (Figure 1), with the examiner briefly covering alternate eyes while the child looks at a toy, may help detect small deviations.9False-positive results are common when children change their fixation because of inattention. False-negative results occur when children are unable to refixate because of amblyopia.

Exotropia is typically an intermittent deviation at first, beginning during the preschool years. As with all cases of strabismus, the deviating eye is at risk of amblyopia, although it is less likely with exotropia than with esotropia. Diagnosis is often a problem because the deviation is most evident when the child looks at something far away. Unfortunately, most primary care offices usually do not have distant objects capable of captivating young childrens' attention. Parents who relate that an eye turns out or that the child closes an eye on a bright day may be describing intermittent exotropia.
Hypertropia and hypotropia, or upward and downward deviations, may be caused by a fourth cranial nerve/superior oblique palsy. Although the deviation may not be apparent on casual inspection, tilting the head to the side of the palsy may cause the affected eye to rise. It is unusual for children to develop strabismus as the only manifestation of underlying neurologic disorders, but acquired deviations related to specific cranial nerve palsies should raise suspicion.
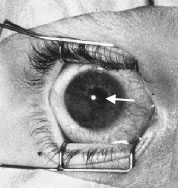
Leukocoria
Alteration in the pupillary light reflexes (called leukocoria if the pupil appears white) may indicate a disorder anywhere within the eye.10 Disorders include corneal opacity, blood (hyphema) or other material in the anterior chamber, cataract, vitreous opacity or retinal disease. The most urgent diagnosis is retinoblastoma (Figure 2), a malignancy most likely arising from retinal germ cells. Because it may be hereditary, a family history of retinoblastoma or of enucleation is of special concern. Although retinoblastoma is almost uniformly fatal without treatment, the cure rate is 90 percent or better when it is promptly recognized and treated,11 and many children can be effectively treated without enucleation.

TESTING FOR THE RED REFLEX
The most useful method of testing for the red reflex is using the ophthalmoscope from a distance of 1 to 2 ft. Sometimes pigmented fundi do not show the reflex well. The examination is best performed in a well-darkened room. If the reflex is still poor, it may be helpful to dilate the pupils with a drop of 1 percent tropicamide (Mydriacyl) or 2.5 percent phenylephrine (Neo-synephrine). Children whose reflexes are still not bright or symmetric should be referred urgently.
Glaucoma
Although glaucoma is usually considered a disease seen in older persons, it also can occur in children. Pressure inside the eye is too high, damaging the optic nerve. Adults with chronic glaucoma typically have minimal symptoms. Children, however, may develop discomfort, light sensitivity, tearing and gradual enlargement or eventually, opacification of the cornea.12 Children who have had cataract surgery are especially at risk for glaucoma,13 even in the absence of symptoms, and should be examined by an ophthalmologist at regular intervals. Also at risk of glaucoma are children with neurofibromatosis and Sturge-Weber syndrome. Pertinent features of congenital glaucoma (which differentiate it from the tearing seen in obstruction of the nasolacrimal duct) include light sensitivity, increased corneal diameter, corneal cloudiness and, occasionally, conjunctival injection. Glaucoma is likely to be bilateral.

Ocular Inflammation
Conjunctivitis is easily treated in most cases. Some children, however, do not respond to topical antibiotics, and may have persistent redness, discharge and discomfort (Figure 3). The most likely cause is probably viral conjunctivitis or keratoconjunctivitis (if the cornea is involved). Most cases are selflimited, but conjunctivitis related to herpes infection can become serious, especially if treated inappropriately with topical corticosteroids. All resistant cases of conjunctivitis require a thorough slit-lamp examination, and it is probably best to avoid using topical medications that include steroids.14,15
On occasion, topical antibiotics may become toxic to the cornea, causing prolonged redness and discomfort. Aminoglycosides are frequent offenders, especially after several days of use. Preparations containing sulfonamides or neomycin are often allergenic. The most effective treatment in such cases is simply to discontinue all medications and observe.
On other occasions, a condition that appears to be conjunctivitis is actually a different kind of ocular inflammation. Disorders of the ocular surface, such as dehydration of the cornea associated with poor eyelid closure or abrasion of the cornea due to misdirected lashes, may cause chronic redness and tearing. Uveitis, or inflammation of the iris, ciliary body or choroid, may also cause light sensitivity, pain and loss of vision.
Uveitis is called iritis if the inflammation is limited to the anterior chamber (Figure 4). The most common cause of iritis is juvenile rheumatoid arthritis. Unfortunately, iritis in children with juvenile rheumatoid arthritis typically has minimal symptoms and is diagnosed on the basis of careful slit-lamp examination. Hence, it is very important that children with iritis have periodic ophthalmologic examinations.
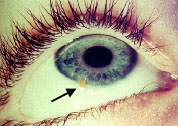
Eye Trauma
Children, especially boys, are at high risk of eye injuries compared with the adult population.16 Corneal abrasions and foreign bodies (Figure 5) cause intense conjunctival redness and sensitivity to light. Topical fluorescein will stain the area of injury and a Wood's lamp may be helpful to visualize the stained area. A foreign body may lodge under the upper lid and cause corneal abrasions with each blink. Projectiles thrown by a lawn mower or dislodged by banging two pieces of metal together may penetrate and enter the eye with minimal external signs. Children with such injuries should be kept on their back with a protective shield over the eye if possible. Such foreign bodies are detected by detailed slit-lamp and fundus examinations and often require imaging studies. Many children with eye trauma, therefore, require referral to an ophthalmologist, initially or in follow-up.
Children with chemical injuries of the eye may present to the primary care office. Whether the offending agent is acid or alkali, the most important treatment is extensive irrigation, preferably with saline or Ringer's lactate solution, begun urgently and continued until a neutral pH is achieved in the tears. The conjunctival cul de sacs should be thoroughly searched for any sequestered particles of caustic material. Subsequently, cycloplegic drops and antibiotic ointment should be prescribed, along with a pressure patch or frequent use of preservative-free artificial tears.
Children with shaken baby syndrome may have retinal and vitreous hemorrhage, which can be detected on ophthalmologic examination. Consultation is indicated if suspicious injuries are seen.
Nystagmus
Children with nystagmus may have disorders of the eye or the central nervous system. The most common cause is probably albinism, which sometimes causes only subtle hypopigmentation of the skin, hair and irides. Ophthalmologic examination with the slit lamp demonstrates the iris pigment defect, as well as retinal hypopigmentation and foveal hypoplasia.
Other children with nystagmus may have bilateral optic nerve hypoplasia (a condition that may be associated with other disturbances of the central nervous system in patients with de Morsier's syndrome), bilateral media opacities or achromatopsia. Children with hearing loss and poor vision should be evaluated for Usher's syndrome, which includes retinitis pigmentosa. Subtle nystagmus may be detected by observing oscillations of the fundus during examination with an ophthalmoscope.
Systemic Conditions
Many other systemic disorders are associated with specific eye findings. For example, homocystinuria and Marfan syndrome may cause dislocated lenses. Patients with Tay-Sachs disease may have a “cherry-red” macula. Cystinosis may be associated with corneal and conjunctival crystals, and a biopsy can be obtained if necessary for diagnosis. The mucopolysaccharidoses may cause corneal clouding.
Final Comment
Family physicians play a crucial role in the management of eye problems in children. Vision screening is a vital part of routine care in children. Even with limited equipment—an interesting toy for fixation, an eye chart, a penlight, a Wood's lamp, fluorescein strips and an ophthalmoscope—family physicians can identify most important causes of vision loss.