Before beginning work on a manuscript, authors should submit an article proposal to afpjournal@aafp.org with the words “Article Proposal for AFP Editor” in the subject line. This allows tailoring of the topic to AFP’s needs and prevents overlap with recently published content or articles in preparation.
Authors must demonstrate expertise in their area of interest or manuscript topic. The most experienced author should take the lead in evaluating the available evidence and writing the manuscript. Article bylines may include a maximum of three contributing authors. In our experience, allowing more than three authors leads to an uneven-quality paper.
Resident physicians must work with an experienced attending physician who serves as the first and corresponding author. Students can be coauthors for only the following departments: Diary of a Family Physician, FPIN’s Clinical Inquiries, FPIN’s Help Desk Answers, Letters to the Editor, Photo Quiz, Practice Guidelines, video submissions, and the AFP Community Blog. Clinical review articles, editorials, and other submissions with student authors are not considered for publication.
When submitting an article proposal, all authors must log into their AAFP account and complete a CME Disclosure Form. If authors do not have an AAFP account, they need to create one to access the CME Disclosure Form.
Note: To avoid bias or the perception of bias, our strict conflict of interest policy precludes us from considering manuscripts sponsored directly or indirectly by a pharmaceutical company, medical education company, or other commercial entity or ineligible company, or those written by an author who has a financial relationship with or interest in any commercial entity or ineligible company that may have an interest in the subject matter of the article within the previous 36 months or in the foreseeable future. This policy also includes serving on a commercial speaker's bureau or advisory board, or receiving commercial research support related to the subject matter of the article, among other relationships outlined in our conflict of interest policy.
Submit articles to Sumi M. Sexton, MD, Editor-in-Chief, using AFP’s ScholarOne submission system. For instructions, see Submitting the Manuscript. Updated information about AFP’s acceptance rates and timelines to publication is also available.
AFP articles are evidence-based clinical reviews. AFP focuses on clinical conditions and diseases that are encountered frequently by practicing family physicians, with an emphasis on diagnosis and treatment. Clinical reviews should be 1,500 to 1,800 words in length.
AFP does not publish original research articles. Although case reports are not featured as articles, brief case summaries may be submitted in the form of a Letter to the Editor (see also Curbside Consultation and Diary of a Family Physician).
Authors are expected to reply to accepted Letters to the Editor and online comments about their article, especially any that question the science involved. Failure to do so may disqualify an author from future publication in AFP.
The AFP Community Blog is an online-only feature that extends discussions of journal content and presents diverse perspectives on clinical, public health, and health policy topics relevant to family medicine. Regular contributors are AFP editors, but guest authors, including residents and students, are welcome.
Blog entries typically range from 400 to 700 words and may include an optional figure or table. Although this format lends itself to a more informal style of writing, clinical recommendations should be supported by references to evidence-based guidelines or studies with patient-oriented outcomes, if available. Sources should be included as hyperlinks in the text. Links to examples of previous entries are available on the AFP Community Blog home page.
Prospective guest authors should submit proposed topics to Kenny Lin, MD, MPH, Deputy Editor at afpjournal@aafp.org.
Curbside Consultation is a feature that addresses legal, psychological, and ethical issues that physicians may encounter in their day-to-day practice. Each piece contains a case scenario with a clinical question, a commentary section, and a resolution of the scenario. Examples are available in the Curbside Consultation department collection.
Authors may submit a topic proposal to Caroline Wellbery, MD, Associate Deputy Editor at afpjournal@aafp.org. If the topic is approved, the author should prepare a brief scenario that describes the challenge to resolve, ending with a clinical question. Although the case is hypothetical, it should be presented as a query to a consultant. The commentary then addresses the pertinent issues presented in the case and should be limited to approximately 1,000 words. The piece should conclude with a resolution of the case scenario, which can include actionable advice for the family physician. One to two small tables (if warranted) can be added, and up to 15 references can be used.
The goal of Diary of a Family Physician is to share experiences and foster a sense of camaraderie among readers. We are looking for stories that provide a real-life flavor of day-to-day practice. These may reflect the broad range of experience in family medicine and diverse clinical settings (e.g., solo or group practice, rural, urban, hospitals, nursing homes, emergency department/urgent care, house calls, telehealth, residency programs, community health centers, universities). Submissions should be sent to afpjournal@aafp.org. Examples are available in the Diary of a Family Physician department collection.
Content may focus on the joys and challenges of everyday family practice, clinical treatment tips, personal experiences with patients and their families, or diagnostic puzzles that can be addressed adequately in the space provided.
Diary submissions should be 150 to 300 words. Six to seven entries should be provided in a submission (representing different hours or patient encounters on a busy day in family medicine with the inclusion of an evening hour if appropriate to describe a longer day or interesting personal or family event). Avoid providing information that might allow anyone to identify a patient. Avoid stories that promote a specific commercial product or political opinions. Diverse perspectives are welcome, but the focus should be on the clinical experience. First person is preferred when referring to yourself, but third person may be acceptable in certain cases, such as when referring to the patient.
Most editorials in AFP are solicited by the editors; however, freestanding editorials are occasionally accepted. Editorials should range from 500 to 800 words in length and may include six to 12 references. Submit editorials as a "Department" manuscript type using AFP's ScholarOne submission system.
Letters to the editor are published in most issues of AFP in print or online only. Online only letters are listed in the print table of contents. Authors may comment on a previously published article or submit a freestanding letter on an important clinical topic. Letters must be submitted in a Word document and be less than 400 words, with a limit of one table or figure, six or fewer references, and no more than three authors. If the letter is in response to a previously published article, that article should be listed as one of the references. Letters must not be submitted to any other publication. Possible conflicts of interest must be disclosed at the time of submission. All authors must log into their AAFP account to complete a CME Disclosure Form. If authors do not have an AAFP account, they need to create one to access the CME Disclosure Form. This form should be completed at the time of their Letter to the Editor submission. On acceptance, authors will be expected to sign a copyright form. Please see our Copyright Transfer policy. If an author of an accepted letter has a conflict of interest that is not deemed to be disqualifying, the editor will add a disclosure statement at the end of the letter.
Submission of a letter grants the AAFP permission to publish the letter in any of its publications in any form. Accepted letters are edited to meet style and space requirements. Send letters to Kenny Lin, MD, Deputy Editor of AFP at afplet@aafp.org.
Photo Quiz presents readers with a clinical challenge based on a photograph or other figure. Submissions should conform to AFP guidelines. Send submissions to afpphoto@aafp.org. Please note that we receive many submissions each month and it can take six to eight weeks for a decision about acceptance.
Photo Quizzes should be original and not published or under consideration for publication elsewhere. Articles that demonstrate a family medicine perspective on and approach to a common clinical condition are particularly desirable.
Authorship:
Images:
Text:
The text of your Photo Quiz should include the following elements: 1) title, 2) introduction paragraph presenting the clinical scenario, 3) a question with one correct and three or four incorrect answers, 4) discussion of correct answer, 5) brief explanation of incorrect answers, and 6) a summary table. The following are specific instructions for each element (view PQ template):
Please review this manuscript checklist carefully before submitting your manuscript to ensure it includes all required components and conforms with AFP style.
In a short paragraph, please succinctly describe your search strategy, the key word(s) used, the date(s) of the search, and the data sources you accessed in identifying the highest-quality evidence on your topic. By "data sources," we mean sources such as Cochrane reviews and Agency for Healthcare Research and Quality, in addition to a PubMed search using the Clinical Query function. Do not list the actual references you found in each source; simply include them in your bibliography.
We strongly recommend that you search the following freely accessible evidence-based sources of information and also consult our Evidence-based Medicine Toolkit.
As part of your paragraph, please also include a statement about the use of individual characteristic classification variables (e.g., race, gender, sexual orientation), if applicable. Please see the sample paragraph below.
If studies used individual characteristic classification variables in analyses or models and you choose to include this information, you should consider the following and clarify in the manuscript: (1) what the variables are truly measuring (i.e., is self-identified race acting as an indicator of systemic racism?); (2) what hypothesis or research question justifies their inclusion; and (3) how the variables were defined/identified in the included studies.
If you believe that there are studies that have important information even though there were questions about how individual characteristic classification variables were identified, please include a statement to that effect in your manuscript. As an example of the limitations inherent in this process, we acknowledge that many studies more than a few years old offered participants only the binary male/female option for gender identity. A brief statement that acknowledges this issue when that study is utilized is acceptable.
The AFP Diversity, Equity, and Inclusion Committee is happy to help with issues like this. Please contact the editor assigned to your manuscript with questions about how to review and evaluate this information in a particular study.
Some examples of how two individual characteristic classification variables, in this case race and gender, are not clearly identified or are identified inappropriately include, but are not limited to, the following:
Sample Data Sources paragraph:
Data Sources: A PubMed search was completed in Clinical Queries using the key terms gout and hyperuricemia. The search included meta-analyses, randomized controlled trials, clinical trials, and reviews. The Agency for Healthcare Research and Quality Effective Healthcare Reports, the Cochrane database, DynaMed, and Essential Evidence Plus were also searched. We critically reviewed studies that used patient categories such as race and/or gender but did not define how these categories were assigned, stating their limitations in the text. Search date: November 18, 2023.
Websites for Sources of Evidence-Based Clinical Information:
Free Access Websites
McMaster University’s compendium of pre-appraised evidence to support clinical decisions. Content is presented in a hierarchical way, with the highest level of available evidence listed first.
Agency for Healthcare Research and Quality
In particular, see AHRQ’s Evidence Reports on clinical topics.
Note: AFP publishes many of these reports in the Implementing AHRQ Effective Health Care Reviews department collection.
Cochrane Database of Systematic Reviews
Free for abstracts only, which in most cases provide the key findings of interest. The complete review requires a subscription. The Cochrane database contains systematic reviews of narrowly focused clinical questions (e.g., colchicine for treating acute gout attacks) as opposed to broad, general reviews of topics (e.g., management of an acute gout attack).
Note: AFP publishes summaries of Cochrane abstracts in Cochrane for Clinicians.
Repository of evidence-based clinical practice guidelines, appraised using the National Academy of Medicine’s Standards for Trustworthy Clinical Practice Guidelines.
National Center for Complementary and Integrative Health
The National Center for Complementary and Integrative Health (NCCIH) conducts research and provides information on complementary and integrative health approaches.
Trip (Turning Research Into Practice)
Contains links to a wide range of journal articles, medical organization clinical guidelines, online medical references, and other sources. A limited version is freely available; additional content requires an annual subscription.
U.S. Preventive Services Task Force
Premier source of evidence-based, graded recommendations for clinical preventive services.
Note: AFP publishes Recommendations and Reports from the USPSTF and CME case studies in the Putting Prevention Into Practice series.
Subscription Required Websites
Most of these are point-of-care clinical information and decision support tools. These websites provide important background information, but authors should review the primary source to use as a citation for the article.
Essential Evidence Plus
Includes POEMS (collections of patient-oriented evidence that matters).
NatMed
Database of dietary supplements, natural medicines, and complementary, alternative, and integrative therapies.
UpToDate
To ensure adequate searching on your topic, we strongly recommend that the above sources be reviewed, in addition to a PubMed search using the Clinical Query function. This is done by using the provided link, or by going to the PubMed home page, and selecting “Clinical queries” from the lower center of the screen.
Manuscripts formatted to conform to the International Committee of Medical Journal Editors Recommendations for the Conduct, Reporting, Editing, and Publication of Scholarly Work in Medical Journals are acceptable for submission.1 AFP endorses these guidelines. Double-space the entire manuscript with 1-inch margins. Arrange the manuscript in the following sequence, with each section beginning on a new page:
The title page, abstract, text, literature search and data sources, references, and tables should be in a single Microsoft Word document (DOC or DOCX). Number pages consecutively in the upper right-hand corner and remove all identifying information.
Please carefully review the detailed instructions for each section that follows:
Please include the following items on the title page:
Sources of support in the form of grants, equipment, or drugs should be disclosed upon submission and when completing a CME Disclosure Form; this information will be included as a footnote to the published article. For details, see AFP’s Conflict of Interest policy.
Include an abstract of 100 to 200 words, depending on the length of the text, that provides factual and specific (rather than general and nonspecific) information summarizing the main points of the manuscript. For example, instead of saying, “This article will describe the differential diagnosis of chest pain in adolescents,” say, “The most common causes of chest pain in adolescents include musculoskeletal strain, hyperventilation syndrome, and anxiety.” For clinical reviews, emphasize key points in the diagnosis and treatment of the condition discussed. All information provided in the abstract should also be available in the body of the article or in tables or figures.
Articles should be 1,500 to 1,800 words (maximum 2,000 words), unless you receive instructions from our editors specifying otherwise. These word counts do not include the title page, abstract, literature search and data sources, references, tables, figures. Manuscripts longer than 2,000 words are rarely accepted.
Do not include a summary or conclusion section; anything that you would ordinarily put in such a section should go in the abstract.
Authors are responsible for citing references accurately and should be able to attest that the references cited support the associated statement. Provide appropriate reference citations to support key clinical recommendations, statistical information, reports of previous studies, controversial statements, etc. Use the following guidelines in choosing references:
Begin the writing process by identifying key clinical questions and controversies related to your topic, and then answer them with the best available evidence. Do not write the article and then find selected references to support your opinions!
Number references in the text in the order of citation. Arrange references numerically, not alphabetically. Do NOT use EndNotes or any other automated reference function.
Abbreviate journal titles according to the style used in PubMed. If there are three or fewer authors, list them all; if there are more than three, list the first three followed by ", et al." Do not use periods after authors’ initials. Include beginning and ending page numbers for journal and book references.
The average number of references for a full-length article ranges from 30 to 40. Most articles should not exceed 50 references.
References first cited in tables or figure legends must be numbered to remain in sequence with references cited in the text.
Reference Examples
Standard Journal Article
Chapter in a Book
Website
Authors should maximize the educational value of tables. Tables should be succinct, as long lists are less helpful. They should be sorted in a clinically meaningful way (e.g., most accurate, most common, most effective) with an explanatory footnote, or otherwise alphabetically if there is not enough data to support a particular order. Provide complete reference data for each item in a table, even if you consider the table to be “original,” and note whether the table has been previously published elsewhere. For all tables that are borrowed or adapted from other sources, include full PDFs of the original sources and ensure that complete reference data are provided. Authors should be prepared to include source information for tables from borrowed sources when they submit their manuscript through ScholarOne.
Do NOT attempt to obtain reprint permission from the original publisher. AFP will seek permission from the copyright owner to publish the material in print and other formats. However, it is possible that the rightsholder will not grant permission for use of copyrighted materials, and AFP reserves the right to withhold tables or figures from print and other formats based on the rightsholder’s terms. We discourage reuse or adaptation of tables from the following sources: JAMA journals, AAP, APA, and UpToDate. Due to the increasing difficulty with obtaining permission to adapt previously published material, we strongly encourage authors to create original tables and figures. See Tips for Creating Original Tables and Algorithms and How to Create an Algorithm in Word.
Tables should be interpretable without reference to the text. Each table should have a title, be numbered sequentially with Arabic numerals (except the SORT: Evidence Table of Key Clinical Recommendations), and be on a separate page.
Use Microsoft Word’s “Tables” function to create the table. Do not just use spaces and tabs, which quickly become misaligned as the manuscript is edited and revised. We also do not accept tables as embedded images (e.g., screenshots). In general, include tables in your main document rather than in separate files.
For tables that include drug pricing, please use information from GoodRx to find representative undiscounted prices, not using GoodRx coupons.
Clinical Decision Tools: Please mention and include links to relevant clinical decision tools and calculators, especially those published in AFP’s Point-of-Care Guides and on the medical calculator website MDCalc.
Costs of laboratory tests, imaging studies, and clinical procedures: Where relevant, please include approximate, representative costs for tests or procedures, especially in tables where comparative cost is discussed. We use Healthcare Bluebook as the source for pricing when possible. If you use another source, please provide a complete citation for it.
Each article should include an evidence table called a SORT or Strength of Recommendations Table. This table helps readers understand the main points of your article, and the strength of evidence that supports its recommendations. The table should contain the key clinical recommendations and strength of recommendation ratings for your article as shown in the example below:
SORT: KEY RECOMMENDATIONS FOR PRACTICE |
||
Clinical recommendation |
Evidence rating |
Comments |
Obtain an ECG in patients presenting with chest pain.1,2 |
C |
Consensus guideline based on observational studies |
Patients with two normal highly sensitive troponin tests an hour apart can safely be sent home.10 |
B |
Meta-analysis of randomized trials |
Patients with chest pain should immediately receive oxygen and if not allergic an aspirin tablet.17,18 |
A |
Consistent findings from randomized controlled trials and recommendation from evidence-based practice guideline |
ECG = electrocardiogram. A = consistent, good-quality patient-oriented evidence; B = inconsistent or limited-quality patient-oriented evidence; C = consensus, disease-oriented evidence, usual practice, expert opinion, or case series. For information about the SORT evidence rating system, go to https://www.aafp.org/afpsort. |
||
The SORT table is intended to highlight the most important three to seven recommendations from your article for clinicians. Each recommendation must be accompanied by a SORT rating of A, B, or C. Your recommendations should emphasize interventions and approaches that improve patient-oriented outcomes (e.g., morbidity, mortality, quality of life) over disease-oriented evidence (e.g., biomarkers, surrogate endpoints).
If you are not comfortable assigning the strength of recommendation (below), please attempt to follow the guidelines but acknowledge your uncertainty and our medical editors will carefully review your work. To rate the strength of evidence supporting key clinical recommendations, please use the following guidelines:
Strength of Recommendation |
Definition |
A |
Recommendation based on consistent and good-quality patient-oriented evidence* |
B |
Recommendation based on inconsistent or limited-quality patient-oriented evidence* |
C |
Recommendation based on consensus, usual practice, expert opinion, disease-oriented evidence,** and case series for studies of diagnosis, treatment, prevention, or screening |
*—Patient-oriented evidence measures outcomes that matter to patients: morbidity, mortality, symptom improvement, cost reduction, and quality of life. |
|
Use the table below to determine whether a study measuring patient-oriented outcomes is of good or limited quality, and whether the results are consistent or inconsistent between studies:
Type of Study |
|||
Study Quality |
Diagnosis |
Treatment/Prevention/Screening |
Prognosis |
Level 1 Good-quality patient-oriented evidence |
Validated clinical decision rule |
Systematic review/meta-analysis of randomized controlled trials (RCTs) with consistent findings |
Systematic review/meta-analysis of good-quality cohort studies |
|
Systematic review/meta-analysis of high-quality studies |
High-quality individual RCT + |
Prospective cohort study with good follow-up |
|
High-quality diagnostic cohort study * |
All or none study ++ |
|
Level 2 Limited-quality patient-oriented evidence |
Unvalidated clinical decision rule |
Systematic review/meta-analysis of lower-quality clinical trials or of studies with inconsistent findings |
Systematic review/meta-analysis of lower-quality cohort studies or with inconsistent results |
|
Systematic review/meta-analysis of lower-quality studies or studies with inconsistent findings |
Lower-quality clinical trial + |
Retrospective cohort study or prospective cohort study with poor follow-up |
|
Lower-quality diagnostic cohort study or diagnostic case-control study * |
Cohort study |
Case-control study |
|
|
Case-control study |
Case series |
Level 3 Other evidence |
Consensus guidelines, extrapolations from bench research, usual practice, opinion, disease-oriented evidence (intermediate or physiologic outcomes only), and case series for studies of diagnosis, treatment, prevention, or screening. |
||
*—High-quality diagnostic cohort study: cohort design, adequate size, adequate spectrum of patients, blinding, and a consistent, well-defined reference standard.
+—High-quality RCT: allocation concealed, blinding if possible, intention-to-treat analysis, adequate statistical power, adequate follow-up (> 80%).
++—An all-or-none study is one where the treatment causes a dramatic change in outcomes, such as antibiotics for meningitis or surgery for appendicitis, which precludes study in a controlled trial.
Consistency Across Studies |
|
Consistent |
Most studies found similar or at least coherent conclusions (coherence means that differences are explainable). or If high-quality and up-to-date systematic reviews or meta-analyses exist; they support the recommendation. |
Inconsistent |
Considerable variation among study findings and lack of coherence. or If high-quality and up-to-date systematic reviews or meta-analyses exist, they do not find consistent evidence in favor of the recommendation. |
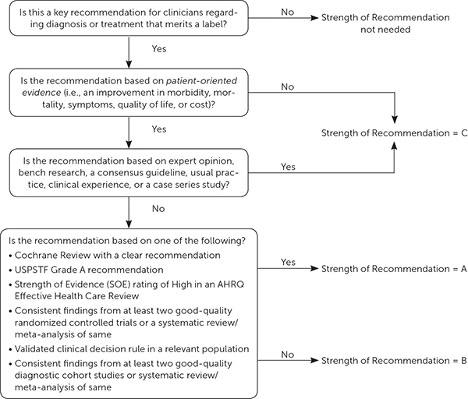
For more information on how to apply these ratings, please see this AFP explanatory article. Use this algorithm for determining the strength of a recommendation based on a body of evidence (applies to clinical recommendations regarding diagnosis, treatment, prevention, or screening). Although this provides a general guideline, authors and editors should adjust the strength of recommendation based on the benefits, harms, and costs of the intervention being recommended.
AFP encourages the submission of original figures that clarify the text. Figures include illustrations, photographs, radiographs, scans, sonograms, diagrams, graphs, flow charts, algorithms, etc. AFP requires authors to transfer copyright ownership of original figures to the AAFP.
Clearly identify figures that have not been previously published and are supplied by a person other than the author and provide complete contact information for the owner of the material. For figures supplied by your institution or a colleague, clearly indicate whether that institution/person is retaining copyright (in which case we will need to contact them) or whether copyright is being transferred to the AAFP.
For all figures that are borrowed or adapted from other sources, include full PDFs of the original sources and ensure that complete reference data are provided. Authors should be prepared to include source information for figures from borrowed sources when they submit their manuscript through ScholarOne.
Do NOT attempt to obtain reprint permission from the original publisher. AFP will seek permission from the copyright owner to publish the material in print and other formats. However, it is possible that the rightsholder will not grant permission for use of copyrighted materials, and AFP reserves the right to withhold tables or figures from print and other formats based on the rightsholder’s terms. Due to the increasing difficulty with obtaining permission to adapt previously published material, we strongly encourage authors to create original tables and figures. See Tips for Creating Original Tables and Algorithms and How to Create an Algorithm in Word.
Each figure should be submitted as a separate file and numbered sequentially as it appears in the text. Diagnostic images (e.g., ECGs, sonograms, radiographs), artwork, line drawings, and nondigital photographs should be scanned at a resolution of at least 600 DPI before submission. Authors should be aware that ScholarOne has a total limit of 350 mb for submission files. Only the following file formats are acceptable; others will be returned to the author for reformatting and resubmission.
Image resolution is typically measured in pixels per inch, or ppi (some use the term "dots per inch," or dpi). The image’s resolution and its dimensions determine the overall file size of the image, as well as the quality of the output. Images with a resolution of 72 ppi (28.35 pixels per cm) are adequate for materials posted on the Web; however, this resolution is inadequate for print media. If your file size is less than 200 kb, it is almost certainly of too low a resolution for a print journal. For color and grayscale images of 3 to 5 inches, we recommend a resolution of 300 ppi (118.11 pixels per cm). Line drawings in black and white require a higher resolution of 600 ppi (236.22 pixels per cm). An image generated by a digital camera as a 72 ppi JPEG file may still be acceptable if it measures at least 14 inches wide or high.
We strongly prefer original photographs/images because images downloaded from websites or taken from other publications rarely reproduce well, even if we are able to obtain permission to reprint them. We also encourage you to consider producing original videos to accompany your article to clarify clinical exams, procedures, etc. Find more information on creating and submitting AFP videos here: https://www.aafp.org/pubs/afp/authors.html#10.
Because the quality of original illustration varies, it may be necessary to have the art you supply redrawn to meet AFP’s artistic standards. AFP’s art department is available to assist authors in the creation of original, high-quality artwork to illustrate manuscripts accepted for publication. This service is provided at no charge to authors but is subject to editorial judgment.
Other guidelines for artwork:
Save each figure as a separate file, with a name that includes the figure number as referenced in the manuscript. Files should be uploaded at the time of manuscript submission in AFP's ScholarOne site and clearly labeled.
Acceptance of a manuscript for publication is contingent on provision of artwork that meets the above specifications. For questions about preparing art or digital images for your manuscript, contact Dave Klemm, AFP Medical Art Coordinator, at afpjournal@aafp.org. After your manuscript has been accepted for publication, address questions about art to the medical editor.
You may acknowledge professional help in the preparation or review of your manuscript. Written permission is required to publish the names of persons acknowledged; see Author Statements. To accommodate blinded peer review, acknowledgments should be submitted in a separate file from the manuscript.
AFP Authors’ Guide Reference
Headings. Use ALL CAPITALS to indicate major sections of the manuscript and Initial Capitals for subsections.
SI Units. Include SI units in parentheses after conventional units (https://academic.oup.com/amamanualofstyle/si-conversion-calculator).
Measurements. Do not include periods after metric measurements.
Numbers. Spell out numbers one through nine. Use numerals for 10 and greater. Exceptions: always use numerals in dosages, percentages, degrees of temperature, and metric measurements.
Drug names. Use the generic name for all drugs. Include the trade name in parentheses after the first mention of a drug in the text. Trade names used in AFP are typically the first brand that was approved. If a drug is not available in the United States, indicate so in parentheses after the drug name.
Abbreviations. Except for units of measurement, abbreviations are discouraged. If used, an abbreviation should be preceded by the words for which it stands. For example, computed tomography (CT). This need only be done on the first use, not throughout the manuscript.
Percentages. Use the percent sign (%) rather than the word “percent.”
Style questions. For questions about medical writing style, consult the American Medical Association Manual of Style.1
Formatting text. Do not justify the right margin; do not use bold print or italics; use a single, standard 12-point typeface (e.g., Times New Roman, Arial); and double-space the entire manuscript.
Reference
AFP is committed to uphold and carry out the work of Diversity, Equity, and Inclusion (DEI), which is part of the mission statement “to empower family physicians to improve the health of patients and communities as the leading source of medical information while advancing science and health equity” and one of AAFP’s key initiatives.
Reflecting DEI in a manuscript can be a complex challenge. Primary questions to consider are “How does this manuscript advance both medical knowledge and health equity?” and “What language and content might help this manuscript avoid perpetuating health disparities?”
Through editorial support, we aim to assist with authors’ efforts to communicate scientific information in a way that is as applicable to as many individuals/settings as possible, to address health disparities in an unbiased way, and to regard author autonomy and preferences.
Language
Examples
Gender-neutral language does not refer to a specific gender or sex (eg, they, chairperson, patients, adults). A gender-additive approach includes gender-neutral language alongside that of womanhood or manhood to avoid excluding any group, especially those who might be disadvantaged (eg, pregnant women and people). Use specific sex or gender terminology as it relates to diagnosis/treatment or where it is otherwise relevant
Example
Person-first language emphasizes the person while viewing the condition as only one part of the whole person (eg, person who is deaf, person experiencing deafness). Identity-first language lists the condition first, which may be preferred by some persons/communities who see the condition as inseparable from their identity (eg, deaf person). Default to person-first language if preference is unknown.
References to race should be capitalized. Refer to race and ethnicity separately because these are not interchangeable terms. When citing research, use the categories as described in the study populations, and acknowledge any limitations of those categories.
Additional resources
Please submit the manuscript as a Microsoft Word document (DOC or DOCX) via AFP’s ScholarOne system.
Please see the Figures section for guidelines on file formats for artwork and photographs. Do not save images within the Microsoft Word or PowerPoint document or use the “Drawing” features of Word.
On manuscript acceptance, authors are required to submit a copyright form that includes an authorship statement, a copyright transfer statement, and an acknowledgment statement. We cannot move forward with publication without this form. In preparation, authors should be aware of our author statements (below) at the time of submission.
To be listed as an author, individuals must have participated sufficiently in the conception and design of the work or the analysis and interpretation of the data, in addition to the writing of the manuscript. Authors must also attest that the manuscript represents valid work and that the manuscript or one with substantially similar content has not been published or is not being considered for publication elsewhere. Finally, authors must take public responsibility for the work. One individual is required to be designated the first and corresponding author, which must not change prior to completion of the manuscript. There can only be a maximum of three individuals listed in the byline for an article. We do not permit medical or other students to serve as AFP authors, except when stated for specific departments. We require that resident physicians, if involved with the article manuscript, work with an experienced attending physician who will serve as lead author and corresponding author.
AFP does not generally permit more than one person to be listed as the first author of an article, a practice known as equal co-authorship. The first and corresponding author is primarily responsible for assuring the accuracy and originality of the submitted manuscript. In addition, the likelihood of two or three co-authors making exactly equal contributions is very small. Please contact the medical editor responsible for your manuscript if you believe that an exception to this policy is warranted.
Each author who was not an employee of the U.S. federal government when this manuscript was prepared must assign, transfer, and convey all rights, title, and interest in the work and its accompanying original tables and figures, including copyright ownership, to the AAFP. All accepted manuscripts become the permanent property of the AAFP and may not be published elsewhere without written permission from the AAFP. Exceptions to this policy apply to the following departments: FPIN-CI, FPIN-HDA, POEMs, and USPSTF.
Each author who was an employee of the U.S. federal government when this manuscript was prepared must specify this on the copyright form, which indicates that the work is not protected by the Copyright Act and there is no copyright of which ownership can be transferred.
The copyright form also includes an acknowledgment statement, which affirms that all persons who have made substantial contributions to the work reported in the manuscript but who are not authors are named in the Acknowledgment section of the manuscript and have given their written permission to be named.
Artificial intelligence technologies (AI), machine learning, and similar technologies, including chatbots like ChatGPT (Chat Generative Pretrained Transformer), have been used in the drafting of scientific manuscripts. Authors who choose to use this technology must disclose at the time of manuscript submission their use of AI, the type of AI utilized, and how they used AI. In addition, when incorporating AI-generated statements, authors must provide correct references in the established literature for all AI-generated items to ensure accuracy and appropriate attribution. AI technology does not qualify for authorship credit, since it cannot guarantee the veracity of the language generated, but its use must be acknowledged in the manuscript.
The AAFP requires all authors to disclose any commercial association that might pose a conflict of interest in connection with the submitted manuscript. All authors complete a CME Disclosure Form and provide additional details upon request if needed to determine whether their submission is selected. If authors do not have an AAFP account, they need to create one to access the CME Disclosure Form.
To avoid bias or the perception of bias, AFP will not consider manuscripts sponsored directly or indirectly by a pharmaceutical company, medical education company, or other commercial entity producing, marketing, re-selling, or distributing health care goods or services to patients or health care professionals or by an ineligible company (as defined by the Accreditation Council for Continuing Medical Education) or written by an author who has or whose spouse/partner has a financial relationship with or interest in any commercial entity or ineligible company that may have an interest in the subject matter of the article within the previous 36 months or in the foreseeable future. This policy includes, but is not limited to, the following relationships/interests:
To avoid writing an article that we will not be able to consider, please contact us first with any questions about this policy. Manuscripts without signed CME Disclosure Forms from all authors will not be considered for peer review.
Note: If you develop, or your spouse/partner develops, new financial relationships with or interests in a relevant commercial entity or ineligible company after initially completing the CME Disclosure Form but before publication, please let us know and complete an updated form immediately. Any such changes may preclude your article from publication.
Advocacy Bias Policy
Certain medical topics are more controversial than others, and therefore run the risk of attracting authors who have strong advocacy positions on the topic, leading to what could be called “advocacy bias.” In this context, “advocacy bias” refers to a strong preference for a position borne out of something other than scientific controversy (i.e., the science is conflicting, and one may reasonably argue for one approach over another), but primarily based on religious, political, social, or other non-medical considerations. In general, we prefer relatively neutral authors who can cover topics in a way that is less subject to this type of bias.
For topics at risk of advocacy bias, authors will be carefully vetted to ensure a relatively neutral presentation, and we may exclude those who we deem to have an undue degree of advocacy bias. However, there are instances in which it is acceptable and even desirable to have “advocacy” authors write for AFP. These include presentations where we specifically address various advocacy viewpoints, such as our series of pro/con editorials, “Controversies in Family Medicine,” or Curbside Consultation. Letters to the Editor are another venue where advocacy authors can be given a platform. All instances are subject to editorial review and approval, as is the case with all our content. More information regarding controversial topics in family medicine and AFP’s approach to such topics can be found in these editorials:
Editorials: Ethics, Education, and American Family Physician
Editorials: Controversial Topics in Family Medicine and Our Duty to Engage
When your manuscript is submitted, the corresponding author receives an automated notification email from ScholarOne that includes the manuscript number and confirmation that the manuscript has been received. Please refer to this number in any communication about your manuscript. Failure to adhere to our Authors’ Guide will cause delays in the processing of your article. Details regarding acceptance rates and publication timelines are available in our annual report.
Manuscripts are reviewed by the editors for suitability and adherence to AFP guidelines. AFP peer review is double-blinded, with acceptable manuscripts reviewed by at least one family physician and one expert in the subject area.
For more information about how to become an AFP peer reviewer and AFP’s peer review standards, see our Reviewers’ Guide.
A decision about acceptance, revision, or rejection is sent to the corresponding author, generally within 10 to 12 weeks of receipt of the manuscript. Acceptable manuscripts require some revision based on reviewers’ comments and medical editor guidance. Instructions showing how to handle each comment and a sample response letter are provided in the Authors’ Responses to Reviews.
Once a manuscript is accepted, it is edited to conform to AFP’s style and improve its educational value. The edited manuscript is sent to the corresponding author for review before publication. Authors are responsible for all statements made in their work, including any changes made by the editors and authorized by the corresponding author. Authors also review a final proof before publication.
Please be considerate and respectful in your communication with AFP staff and medical editors, including being responsive to queries from our editors and replying in a timely manner. We take many factors into consideration when deciding whether to invite authors to write for AFP again. Although our top priority is producing high-quality content for our readers, the failure of any author to comply with these requests of professionalism may result in not being reinvited to write for AFP.
Videos help expand the knowledge and expertise of AFP’s readers. Videos can be freestanding or accompany clinical review articles. All videos are peer-reviewed by at least two medical editors and, if accepted, are published on the AFP YouTube channel. Videos are promoted on the AFP's Video Collection Page, which receives 2.5 million unique visitors each month and 31 million unique visitors each year, including from AAFP members.
We are seeking original, high-quality, concise, clinically impactful videos that teach office procedures, physical examination skills, and clinical findings. We consider existing videos and welcome proposals for videos on new topics. The first author of the video must be an experienced physician. Residents and medical students may be coauthors. We cannot provide financial support or equipment.
Seek approval for your submission by sending a completed video proposal form to Chris Bunt, MD, at afpvideos@aafp.org.
Once approved, submit your video to afpvideos@aafp.org using a common, cloud-based service (e.g., Google Drive, OneDrive). Include a Word document containing the video title, a plain language description of the video, and a copyright transfer form. Completed consent forms are required from anyone appearing in the video (e.g., physicians, patients).
Delete or obscure any identifying information about the patient, hospital, or health care system, including the date. Our goal is to avoid commercialization of any product, hospital system, or institution. When referring to drugs or devices, use generic names or descriptions.
The video file should be complete, in final format, and at as high a resolution as possible. Any editing is the authors’ responsibility, and AFP staff may request additional edits following peer review. AFP staff may abridge the video for content, length, or quality.
Submit your video in a mpeg or QuickTime (.mov) format. If possible, include a still image from the video for use in print or on a nonanimated website page.
{kind=link}