
Am Fam Physician. 2015;91(10):698-706
Author disclosure: No relevant financial affiliations.
Neck masses are often seen in clinical practice, and the family physician should be able to determine the etiology of a mass using organized, efficient diagnostic methods. The first goal is to determine if the mass is malignant or benign; malignancies are more common in adult smokers older than 40 years. Etiologies can be grouped according to whether the onset/duration is acute (e.g., infectious), subacute (e.g., squamous cell carcinoma), or chronic (e.g., thyroid), and further narrowed by patient demographics. If the history and physical examination do not find an obvious cause, imaging and surgical tools are helpful. Contrast-enhanced computed tomography is the initial diagnostic test of choice in adults. Computed tomography angiography is recommended over magnetic resonance angiography for the evaluation of pulsatile neck masses. If imaging rules out involvement of underlying vital structures, a fine-needle aspiration biopsy can be performed, providing diagnostic information via cytology, Gram stain, and bacterial and acid-fast bacilli cultures. The sensitivity and specificity of fine-needle aspiration biopsy in detecting a malignancy range from 77% to 97% and 93% to 100%, respectively.
The primary concern in adults with a persistent neck mass is malignancy. Fortunately, a history and physical examination coupled with an organized diagnostic evaluation typically reveal a definitive diagnosis. When the etiology is elusive, a head and neck surgeon should be consulted.
| Clinical recommendation | Evidence rating | References |
|---|---|---|
| A persistent neck mass in an adult older than 40 years should prompt a search for a malignant source. | C | 1, 6, 8, 10 |
| Contrast-enhanced computed tomography is the initial diagnostic test of choice in an adult with a persistent neck mass. | C | 20 |
| Fine-needle aspiration biopsy is an effective tool to determine the etiology of a neck mass. | C | 7, 13, 14, 21 |
Anatomic Considerations
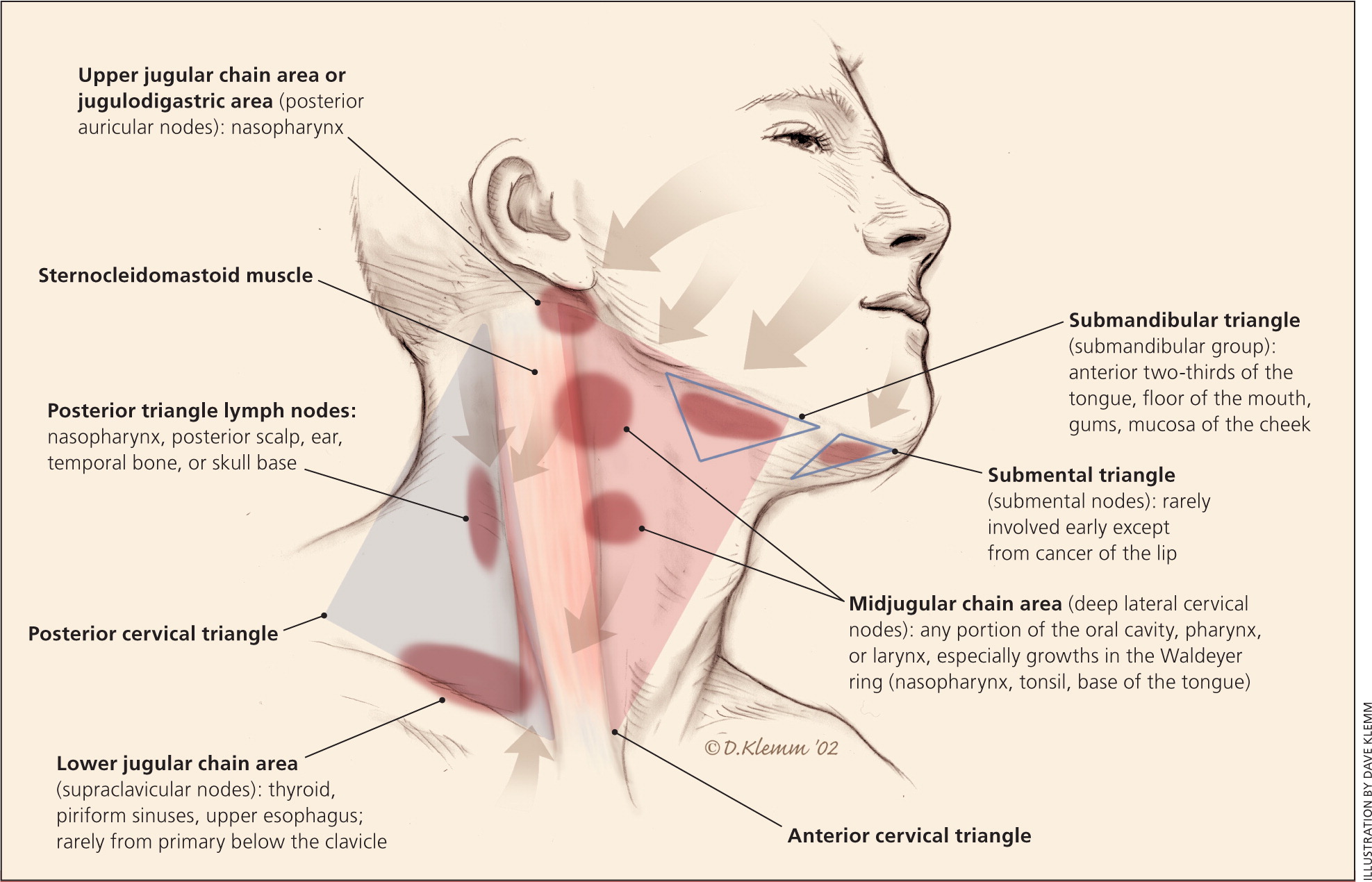
Neck anatomy is divided into triangles with the sternocleidomastoid being the central component of each division. The anterior and posterior cervical triangles share a common border with the sternocleidomastoid. The common pattern of lymphatic drainage is helpful in diagnosing metastases from various organs (Figure 1).
Differential Diagnosis
| Type | Common | Uncommon | Rare |
|---|---|---|---|
|
|
| |
|
|
|
|
|
|
|
|
| Condition | History/risk factors | Physical findings | Diagnosis | Management | |
|---|---|---|---|---|---|
| Acute | |||||
| Acute sialadenitis | Older, debilitated persons with dehydration or recent dental procedures | Rapid or gradual onset of pain and swelling; local edema, erythema, tenderness, or fluctuance consistent with an abscess | Contrast-enhanced CT | Sialagogues, gentle massage; abscess, express by compressing the gland | |
| Hematoma | Trauma | Soft, possible overlying ecchymosis | Ultrasonography or contrast-enhanced CT | Monitor if small; surgical drainage if large or expanding | |
| Pseudoaneurysm or arteriovenous fistula | Trauma with shearing forces | Lateral; soft, pulsatile mass with a thrill or bruit | CT with or without CT angiography | Surgical evaluation for ligation | |
| Reactive lymphadenopathy | |||||
| Bartonella henselae infection | Kitten or flea exposure | Isolated, mobile, fluctuant, tender, warm, erythematous, > 2 cm near site of inoculation | Bartonella antibody titers | Azithromycin (Zithromax) | |
| Cytomegalovirus | URI symptoms | Rubbery, mobile, cervical, and generalized; > 2 cm | Cytomegalovirus titer | Biopsy if no resolution after 8 weeks | |
| Epstein-Barr virus infection | URI symptoms | Rubbery, mobile, cervical, and generalized; > 2 cm | Monospot, Epstein-Barr virus titer | Biopsy if no resolution after 8 weeks | |
| HIV infection | Blood/sexual contact | Rubbery, mobile, cervical, and generalized | HIV enzyme-linked immunoassay | Highly active antiretroviral therapy | |
| Mycobacterium tuberculosis (extrapulmonary) | Travel to or immigration from an endemic area, homelessness, immunocompromise | Diffuse, bilateral lymph nodes (multiple, fixed, firm, nontender) | Purified protein derivative test to rule out atypical mycobacteria infection; acid-fast bacilli culture | Antibiotics: rifampin and isoniazid; add pyrazinamide and ethambutol or streptomycin in endemic areas; refer to a head and neck surgeon if persistent after initial diagnosis and treatment | |
| Staphylococcal or streptococcal infection | Skin infections | Mobile, fluctuant, tender, warm, erythematous | Clinical | Antibiotics | |
| Toxoplasmosis | Cat feces exposure | Rubbery, mobile, cervical, and generalized | Toxoplasmosis antibody titer | Supportive care or treat with pyrimethamine and sulfadiazine | |
| Viral URI | URI symptoms | Mobile, rubbery, bilateral; subsides in 3 to 6 weeks | Clinical | Biopsy if no resolution 3 to 6 weeks after symptom resolution | |
| Subacute (weeks to months) | |||||
| Cancer | |||||
| Hodgkin lymphoma | 15 to 34 years of age and > 55 years, constitutional symptoms, later splenomegaly | Painless, rapidly growing lymph node; rubbery, soft, mobile | Contrast-enhanced CT of the neck, chest, abdomen, pelvis; biopsy | Refer to oncology | |
| Human papillomavirus–related squamous cell carcinoma | 35- to 55-year-old white men with a history of smoking, heavy alcohol use, and multiple sex partners (especially involving orogenital contact) | Rapidly enlarging, lateral, cystic lymph nodes; persistent cervical nodal hypertrophy; palatine or lingual tonsillar asymmetry; dysphagia; voice changes; pharyngeal bleeding | Nasal endoscopy, laryngoscopy, bronchoscopy with biopsies | 2-week trial of antibiotics; refer for biopsy if no resolution | |
| Metastatic cancer | History of melanoma or lung, breast, colon, genitourinary cancer | Matted, firm, fixed lymph nodes | Contrast-enhanced CT of the neck, thorax, abdomen, pelvis | Refer to oncology | |
| Non-Hodgkin lymphoma | Older persons | Painless, rapidly growing lymph node; rubbery, soft, mobile; may involve the tonsillar ring in the pharynx | Contrast-enhanced CT of the neck, chest, abdomen, pelvis; biopsy | Refer to oncology | |
| Parotid tumors | Asymptomatic | Slow-growing, unilateral, mobile, asymptomatic; cranial nerve (often VII [facial]) involved if malignant | Contrast-enhanced CT and/or FNAB | Refer to ENT for excisional biopsy | |
| Upper aerodigestive tract squamous cell carcinoma | Male sex; use of tobacco, alcohol, betel nut | Nonhealing ulcers, dysarthria, dysphagia, odynophagia, loose or misaligned teeth, globus, hoarseness, hemoptysis, oropharyngeal paresthesias | Nasal endoscopy, laryngoscopy, bronchoscopy with biopsies | 2-week trial of antibiotics; refer for biopsy if no resolution | |
| Chronic sialadenitis | Mild to severe pain, often after meals | Firm gland | CT | Sialagogues, gentle massage, refer to ENT | |
| Idiopathic diseases | |||||
| Castleman disease (angiofollicular lymphoproliferative disease) | Constitutional symptoms | Solitary lymph node | Contrast-enhanced CT (shows no enhancement, unlike lymphoma); FNAB | Refer to hematology | |
| Kikuchi disease (histiocytic necrotizing lymphadenitis) | Lymphadenopathy, fever, leukopenia | Posterior lymphadenopathy resolves in 3 months | FNAB | Refer to hematology | |
| Kimura disease | Endemic in Asia; painless subcutaneous mass, eosinophilia | Submandibular triangle, orbital, epicranial, periauricular; nontender, ill-defined | Eosinophilia, elevated immunoglobulin E level, biopsy | Refer to hematology | |
| Rosai-Dorfman disease | Occasional fever in healthy young adults | Matted lymphadenopathy | Elevated erythrocyte sedimentation rate, polyclonal hypergammaglobulinemia | Refer to hematology | |
| Systemic diseases | |||||
| Amyloidosis | Asymptomatic or associated CHF, nephrotic syndrome, neuropathy | Painless systemic lymphadenopathy | FNAB or excisional biopsy | Refer to hematology | |
| Sarcoidosis | 20- to 40-year-old black persons, variable presentation: persistent cough, skin rash/patch, joint pain, arrhythmias | Painless cervical, axillary, inguinal lymphadenopathy | FNAB or excisional biopsy; chest radiography or CT | Refer to pulmonary/rheumatology if necessary | |
| Sjögren syndrome | Xerophthalmia, xerostomia | Parotid gland enlargement | Antinuclear antibodies, SS-A and SS-B antibodies, FNAB | Symptomatic treatment with sialagogues, frequent water intake | |
| Chronic (usually evident as long-standing) | |||||
| Carotid body tumors | Flushing, palpitations, hypertension if hormonally active, dysphagia, dyspnea, eustachian tube dysfunction | Painless oropharyngeal or upper anterior triangle of the neck; pulsatile, compressible with a bruit or thrill, mobile from medial to lateral direction | CT, CT angiography (lyre sign); plasma and urine metanephrines, catecholamines | Refer to ENT | |
| Congenital cysts | |||||
| Branchial cleft cyst | Often diagnosed as a child; slow or rapidly growing after URI; acute or subacute | Mandibular angle, anterior to sternocleidomastoid | Ultrasonography | Antibiotics; refer to ENT for excision after repeated infections | |
| Dermoid cyst | Children and young adults | Submental triangle; soft, doughy, painless | CT | Surgical excision | |
| Thyroglossal duct cyst | Often diagnosed in childhood; slow growing or may arise quickly after URI; may present as acute or subacute | Midline, adjacent to the hyoid bone; rises with deglutition | CT (assures no thyroid cancer calcifications) | Antibiotics; refer to ENT for excision after repeated infections | |
| Glomus vagale, glomus jugulare tumors | Flushing, palpitations, hypertension if hormonally active, dysphagia, dyspnea, eustachian tube dysfunction | Similar to carotid body tumors; ipsilateral tonsil may pulsate and be deviated to midline | CT, plasma and urine metanephrines, catecholamines | Refer to ENT | |
| Goiters (enlarged thyroid) | |||||
| Graves disease | Hyperthyroid symptoms | Associated exophthalmos, pretibial myxedema | TSH-receptor antibody; diffuse uptake on scintigraphy | Radioactive iodine ablation, thyroidectomy, methimazole (Tapazole) or propylthiouracil | |
| Hashimoto thyroiditis | Hypothyroid symptoms | Enlarged thyroid | Thyroid peroxidase antibody | Levothyroxine | |
| Iodine deficiency | Reduced dietary iodine; exposure to thiocyanate (cassava, various vegetables) | Diffusely enlarged thyroid | Dietary history | Increase iodine/decrease thiocyanate containing compounds | |
| Lithium use | Bipolar disease | Diffusely enlarged thyroid/rare nodular thyroid | History of exposure | Monitor thyroid function at 6 to 12 months, treat dysfunction, discontinuation not required | |
| Toxic multinodular | Hyperthyroid symptoms | Diffusely nodular | Multiple foci on scintigraphy | Radioactive iodine ablation, thyroidectomy, methimazole or propylthiouracil | |
| Laryngocele | Repetitive nose blowing, coughing, or blowing into a musical instrument | Midline, superior to thyroid cartilage; resonant, intermittent, globus sensation | CT or laryngoscopy | Refer to ENT | |
| Lipomas | Age > 35 years, possible history of trauma | Soft, mobile, discrete subcutaneous tumors | CT | Monitor or excise | |
| Liposarcoma | Middle-aged | Slowly enlarging, painless, nonulcerated or rapidly growing and ulcerated | CT; excisional biopsy | Excision | |
| Parathyroid cysts or cancer | Hypercalcemia symptoms, family history of multiple endocrine neoplasia | Anterior cervical triangle | Serum calcium, parathyroid hormone immunoassay | Refer to endocrinology, ENT | |
| Thyroid nodules | |||||
| Cold thyroid nodule | Usually asymptomatic | Solitary nodules | TSH, FT4, thyroid ultrasonography, FNAB if > 1 cm | Refer to endocrinology, repeat ultrasonography in 6 to 18 months | |
| Thyroid cancer | Radiation, childhood lymphoma, family history, age < 45 years, hoarseness | Solitary nodules | TSH, FT4, thyroid ultrasonography, FNAB if > 1 cm | Refer for excision | |
| Toxic thyroid adenoma | Hyperthyroid symptoms | Solitary nodules | TSH, FT4, thyroid ultrasonography, FNAB if > 1 cm | Radioactive iodine or thyroidectomy | |
ACUTE NECK MASSES
Neck masses that appear over a short period are generally symptomatic. Blunt or sharp trauma may damage tissue and vasculature, creating a hematoma. Small hematomas are typically self-limited, but large, rapidly expanding hematomas require immediate intervention and possible surgical exploration. Similar mechanisms of trauma, plus the addition of shearing forces, potentiate the formation of pseudoaneurysms or arteriovenous fistulas characterized by soft, pulsatile masses with a thrill or bruit. Computed tomography (CT) angiography delineates the extent of any possible vascular injury, and treatment is usually surgical ligation.1
By far, the most common cause of cervical lymphadenopathy is infection or inflammation created by an array of odontogenic, salivary, viral, and bacterial etiologies. These lymph nodes are often swollen, tender, and mobile, and can be erythematous and warm. Upper respiratory symptoms caused by common viruses usually last for one to two weeks, whereas lymphadenopathy generally subsides within three to six weeks after symptom resolution.2 Although unknown viruses cause 20% to 30% of upper respiratory infections, which occur an average of two to four times per year in adults, more common viral pathogens include rhinoviruses, coronaviruses, and influenza.3,4 Biopsy is appropriate if an abnormal node has not resolved after four to six weeks, and should be performed promptly in patients with other findings suggestive of malignancy, such as night sweats, fever, weight loss, or a rapidly growing mass.5 Certain infectious etiologies (human immunodeficiency virus [HIV], Epstein-Barr virus, cytomegalovirus, toxoplasmosis) tend to cause generalized lymphadenopathy, which emphasizes the need for a comprehensive lymph node evaluation.1
Bacterial infections of the head and neck predominantly cause cervical lymphadenopathy. Lymphadenopathy caused by Staphylococcus aureus or group A beta Streptococcus has no predictable sites of lymph node inflammation. Disseminated Epstein-Barr virus or HIV infection often involves the cervical chain.2 Common antibiotics used for lymphadenopathy include first-generation cephalosporins, amoxicillin/clavulanate (Augmentin), or clindamycin.
Bartonella henselae infection causes mobile, fluctuant, erythematous, and tender, but characteristically isolated, lymph nodes similar to lymphadenopathy caused by staphylococcal and streptococcal infections. Cat-scratch disease develops when a kitten or flea transmits B. henselae, producing a regional lymphadenopathy, usually near the site of inoculation.1,2
The extrapulmonary form of Mycobacterium tuberculosis infection causes a cervical lymphadenopathy. The diffuse, bilateral lymph nodes are characteristically multiple, fixed, firm, nontender masses located in the posterior triangle/cervical chain.1 Suspicion should be high in those who have recently immigrated from or traveled to tuberculosis-endemic areas such as India, Southeast Asia, or sub-Saharan Africa, and purified protein derivative testing should be performed in these patients. A negative result on purified protein derivative testing does not rule out atypical mycobacterial infections, which also should be considered. A fine-needle aspiration biopsy (FNAB) of the lymph nodes or referral to a head and neck surgeon may be warranted if the lymphadenopathy persists after initial diagnosis and treatment.
Inflammation of salivary glands (acute sialadenitis) commonly occurs in older, debilitated persons in the setting of dehydration or recent dental procedures.1 Affected salivary glands cause rapid or gradual onset of pain and swelling, possibly with local edema, erythema, and tenderness or fluctuance consistent with an abscess. Bimanual compression toward the duct opening may expel purulent discharge into the oral cavity. Neck CT with intravenous contrast media may be warranted to confirm this diagnosis and rule out other contributing etiologies such as a dental abscess or local tumor compression.1
SUBACUTE NECK MASSES
Subacute masses are noticed within weeks to months. Although these masses might grow somewhat quickly, they often go unnoticed at onset because of their asymptomatic nature. A persistent asymptomatic neck mass in an adult should be considered malignant until proven otherwise.6 Because delayed diagnosis contributes to decreased survival in conditions such as laryngeal cancer, it is paramount for family physicians to recognize common presentations of head and neck cancers.7,8
Squamous cell carcinomas of the upper aerodigestive tract are the most common primary neoplasms of the head and neck, and their metastases are often the source of cervical lymphadenopathy of unknown origin.8 Common presenting symptoms include nonhealing ulcers, dysarthria, dysphagia, odynophagia, loose or misaligned teeth, globus, hoarseness, hemoptysis, and oropharyngeal paresthesias.8 Lymph nodes associated with malignancy are usually firm, fixed, and matted. However, any persistent cervical lymphadenopathy or symptoms in the setting of risk factors, nonresponse to antibiotics, or unclear etiology warrants further investigation.7 Risk factors for upper aerodigestive tract cancers include male sex and use of alcohol, tobacco, or betel nut (commonly chewed by Southeastern Asians).8 Additional risk factors for oropharyngeal cancer include a family history of squamous cell carcinoma of the head and neck and poor oral hygiene.9
A subset of squamous cell carcinomas with increasing prevalence includes those related to human papillomavirus infection (especially high-risk human papillomavirus 16).9,10 These lesions present with rapidly enlarging, lateral, cystic lymph nodes; persistent cervical nodal hypertrophy; palatine or lingual tonsillar asymmetry; dysphagia; voice changes; or pharyngeal bleeding.10 The population most at risk is 35- to 55-year-old white men with a history of smoking, heavy alcohol use, and multiple sex partners (especially involving orogenital contact).9
Nearly 80% of salivary gland tumors are benign and arise in the parotid gland.1 These tumors are unilateral, asymptomatic, slow-growing, mobile masses, in contrast to malignant tumors, which may have rapid growth, skin fixation, pain, or cranial nerve involvement (especially cranial nerve VII [facial]).1,11 An intraparotid or isolated pre-auricular lymph node is another diagnostic possibility. Excisional biopsy is the preferred diagnostic approach for these tumors following review of contrast-enhanced CT or FNAB results.11 Persistent glandular enlargement with symptoms of xerophthalmia and xerostomia may point to Sjögren syndrome, whereas a hypertrophied, fibrotic gland may suggest chronic sialadenitis caused by a duct stone (sialolith) or stenosis.12
Skin cancers, especially melanoma, also metastasize to local lymph nodes. When a primary head and neck cancer is not evident to explain regional lymphadenopathy, physicians should search mucosal areas (nose, paranasal sinuses, oral cavity, and nasopharynx) for melanoma.7 Rarely, metastases from basal cell and squamous cell carcinoma lead to lymphadenopathy.7 Constitutional symptoms of fever, chills, night sweats, and weight loss may point to distant metastases. When metastases manifest as supraclavicular lymphadenopathy, FNAB reveals a malignancy in more than one-half of cases, with age older than 40 years being the major predictor of malignancy.13 The most common primary malignancy sites that produce cervical lymphadenopathy include the lungs, breasts, lymphomas, uterine cervix, gastroesophageal area, ovaries, and pancreas.13
The neck is a common area for lymphoma to present as a painless lymph node that may grow rapidly, and subsequently become painful. Early constitutional symptoms often precede development of diffuse lymphadenopathy and splenomegaly. In comparison to lymph nodes associated with metastatic disease characterized above, those associated with lymphoma are usually rubbery, soft, and mobile.11 Hodgkin lymphoma has a bimodal age distribution (15 to 34 years and older than 55 years)14 and rarely presents extranodally, whereas non-Hodgkin lymphoma is more common in older adults and is likely to present extranodally in the tonsillar ring located in the pharynx.1 Contrast-enhanced CT of the neck, chest, abdomen, and pelvis helps stage the lymphoma and provides possible biopsy sites.1
CHRONIC NECK MASSES
Congenital masses are more common in childhood but can grow slowly, persisting into adulthood. Thyroglossal duct cysts, the most common congenital cyst, are midline, adjacent to the hyoid bone, and rise with deglutition. These cysts are normally recognized by five years of age, with 60% diagnosed by 20 years of age. However, in one autopsy series, thyroglossal duct cysts were present in 7% of adults, although most were not clinically apparent. Branchial cleft cysts usually present anterior to the sternocleidomastoid muscle, and represent 22% of congenital neck masses.16 Patients may describe a discrete, tender, erythematous mass, which often coincides with recurrent upper respiratory symptoms. Dermoid cysts, typically located in the submental triangle, are soft, doughy, painless masses that enlarge with entrapment of epithelium in deeper tissue and are less prevalent than thyroglossal or branchial cleft cysts.16
Similar to treatment for bacterial lymphadenopathy discussed earlier, empiric antibiotic coverage for staphylococcal, streptococcal, and gram-negative anaerobe pathogens using first-generation cephalosporins, amoxicillin/clavulanate, or clindamycin is appropriate in the initial management of a presumed congenital cyst infection.2 Excision is the definitive treatment for these cysts and tracts and may be considered after repeat infections.
Thyroid pathology accounts for most chronic anterior neck masses, and these masses are often insidious. A diffusely enlarged thyroid gland may be due to Graves disease, Hashimoto thyroiditis, or iodine deficiency, but can be caused by goitrogenic exposures such as lithium.6 Thyroid nodules are common, with an estimated prevalence of 4% to 7% in adults; only 5% of these are malignant.1 Physical examination is unreliable in detecting nodules smaller than 1 cm.6 A review of thyroid nodules was recently published in American Family Physician.17
A laryngocele may also develop in the anterior triangle as a traumatic neck mass created by chronic coughing or repetitive blowing (e.g., from nose blowing or blowing into a musical instrument), which causes herniation of the laryngeal diverticulum through the lateral thyrohyoid membrane. Increased airway pressure causes an intermittent air-filled swelling of the neck that is resonant to percussion. The swelling can potentially become a laryngopyocele, which can obstruct the airway.18 Contrast-enhanced CT or laryngoscopy can confirm a laryngocele or laryngopyocele, which requires surgical excision.19
Paragangliomas are neuroendocrine tumors involving the chemoreceptors of the carotid body, jugular vein, or vagus nerve in the lateral neck. Carotid body and glomus jugulare tumors commonly present in the upper anterior triangle near the carotid bifurcation as a pulsatile, compressible mass with a bruit or thrill.11 Although mobile from medial to lateral direction, these tumors are fixed in the cranial to caudal plane. They are usually asymptomatic, but when functional they cause flushing, palpitations, and hypertension as a result of catecholamine release. Diagnostic testing includes plasma or 24-hour urine collection for catecholamines and metanephrines.1
Diagnostic Approach
The initial diagnostic test of choice in an adult with a persistent neck mass is contrast-enhanced CT,20 which provides valuable initial information regarding the size, extent, location, and content or consistency of the mass. Additionally, contrast media may help identify malignant lymph nodes that are not enlarged and distinguish vessels from lymph nodes.20
Table 3 shows the preferred imaging modalities for neck masses and lymphadenopathy according to American College of Radiology Appropriateness Criteria.20 Of note, contrast can obscure visualization of sialoliths, and non–contrast-enhanced CT is recommended for suspected swollen salivary glands due to sialolith obstruction.20 Iodine-based contrast media should be avoided in patients with a history of thyroid disease or when metastatic thyroid cancer is a concern.20 Although positron emission tomography (PET) with CT can be used to distinguish between malignant and unaffected tissues, its use in the preliminary diagnosis is not as effective and should be limited to definitive management of a malignancy.20
| Scenario | Recommended test | Comments |
|---|---|---|
| Nonpulsatile solitary mass or multiple neck masses | Contrast-enhanced CT | — |
| Pulsatile neck mass | Contrast-enhanced CT and contrast-enhanced CT angiography | May be performed at the same time |
| Patient with a neck mass and history of cancer treatment | Contrast-enhanced CT or CT with positron emission tomography | Positron emission tomography is superior in this subset of patients |
When ultrasonography is indicated instead of or in addition to CT, it is useful to distinguish cystic from solid lesions, detect nodal size, and differentiate high-flow from low-flow vascular malformations.20 Ultrasonography may also be helpful in guiding FNAB of nonpalpable or small superficial lesions.20 Although CT and ultrasonography share similar capabilities, ultrasonography is often preferred initially in younger patient populations to reduce radiation exposure. It may also be preferred to avoid contrast media–induced nephropathy in patients with underlying renal disease.
CT angiography is recommended for evaluating a pulsatile neck mass and is preferred over magnetic resonance angiography (MRA).20 CT, MRA, and PET with CT are all useful in the evaluation of patients after cancer treatment. PET with CT appears to be superior to MRA or CT for detecting recurrent tumors, but it should be considered only on request from the surgical oncology team.20
The clinician may proceed with FNAB, if indicated, once appropriate imaging has ruled out involvement of underlying vital structures. FNAB can provide further information through cytology, Gram stain, and bacterial and acid-fast bacilli cultures while avoiding complications of open biopsy. The sensitivity of FNAB for detecting a malignancy ranges from 77% to 97%, and the specificity ranges from 93% to 100%.7,13,14,21 FNAB should never be performed on a pulsatile mass or a mass that appears to be vascular in origin.
Patients with suspected infectious and inflammatory masses should be tested for HIV, Epstein-Barr virus, cytomegalovirus, toxoplasmosis, tuberculosis, and B. henselae, when clinically appropriate. Endocrine masses can be assessed further with blood work, including thyroid and parathyroid hormone panels. Visualization with laryngoscopy, bronchoscopy, or esophagoscopy may have an important role in further evaluation of neck masses that are not adequately characterized by ultraso-nography, contrast-enhanced CT, or FNAB.
Data Sources: A PubMed search was completed in Clinical Queries using the key terms neck mass, diagnosis, and adult. The search included meta-analyses, randomized controlled trials, clinical trials, and reviews. We also searched the Agency for Healthcare Research and Quality evidence reports, Clinical Evidence, the Cochrane database, Essential Evidence Plus, the Institute for Clinical Systems Improvement, the National Guideline Clearinghouse database, Family Physicians Inquiries Network, and the TRIP database. Search dates: August 30, 2014, and January 19, 2015.
