
Am Fam Physician. 2013;88(11):771-772
Author disclosure: No relevant financial affiliations.
A 38-year-old man presented with a painful rash on his right ear that had lasted for seven days. Over the previous four days, he developed ipsilateral tinnitus and progressive difficulty in closing his right eye and mouth. He had no notable medical history.
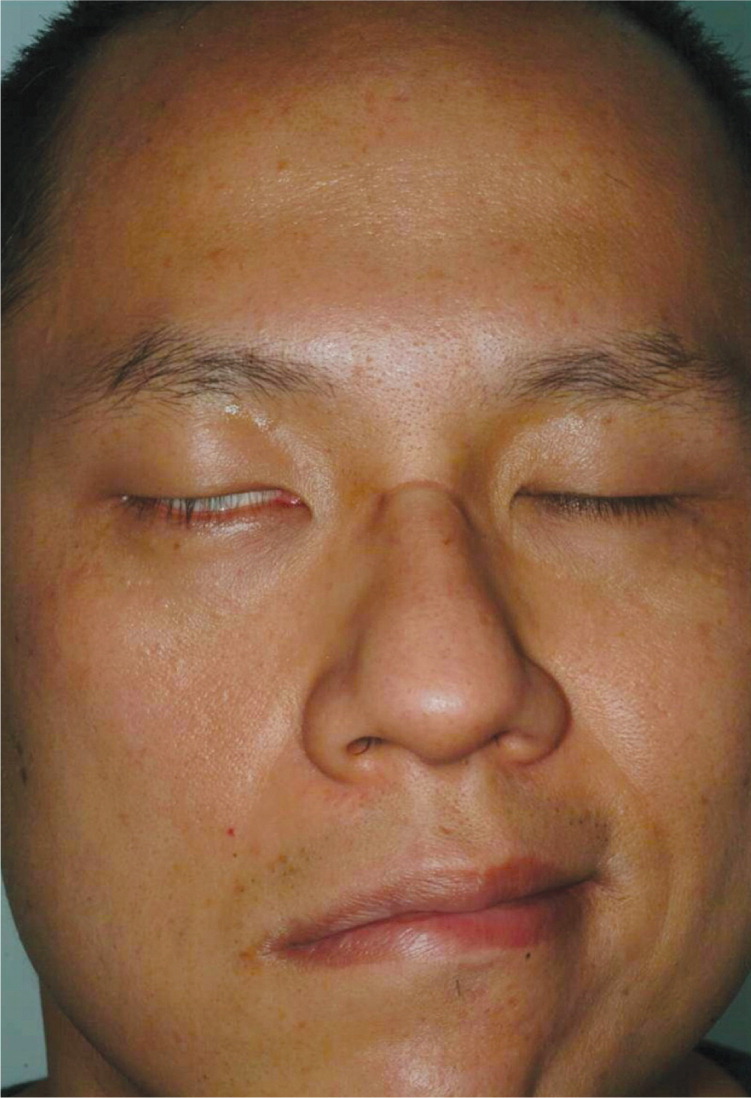
On examination, he had multiple vesicles on an erythematous base on the concha of his right ear (Figure 1). Neurologic examination showed right-sided hearing impairment and lower motor neuron facial palsy with lagophthalmos, an inability to smile on the affected side, and loss of definition in the right nasolabial fold (Figure 2).

Question
Discussion
The answer is D: Ramsay Hunt syndrome, or herpes zoster oticus, is characterized by herpes zoster infection of the external ear or tympanic membrane with involvement of the facial and/or auditory nerves.1 The clinical manifestation includes unilateral peripheral facial palsy, with or without tinnitus, vertigo, or deafness.1,2 Ramsay Hunt syndrome can usually be diagnosed based on clinical findings.1 A Tzanck smear of the vesicular fluid can be performed to evaluate for multinucleated giant cells, which are indicative of varicella or herpes zoster infection.1,2 A viral culture is generally not required, but can differentiate between varicella and herpes simplex virus.1
Initiation of antiviral therapy within 72 hours of rash onset leads to the best outcomes in most adults.1,3–5 However, less than 50% of patients achieve complete neurologic recovery.1 Topical antiviral therapy is effective against cutaneous infection of herpes simplex virus but is not effective on the herpes zoster rash.1 The use of systemic corticosteroids is controversial, but may be considered for healthy older adults with severe pain and no contraindications.1 The pain of herpes zoster can be a significant problem, especially in older persons.1,3,5 Most patients experience pain during the acute phase that requires regular analgesics. Occlusive ointments and creams or lotions containing corticosteroids should be avoided.1
Bell palsy is a common cause of facial drooping. Patients present with unilateral facial weakness, difficulty closing an eye, and loss of furrows in the brow. Most cases are idiopathic and will resolve spontaneously.6
Neurosarcoidosis occurs in 5% to 10% of patients with sarcoidosis. The most common clinical manifestation of neurosarcoidosis is a bilateral or unilateral seventh cranial nerve palsy, although other cranial nerve palsies are possible. The condition usually resolves spontaneously but may recur, possibly years after the initial presentation.
Parry-Romberg syndrome is a rare progressive unilateral facial atrophy. It is thought to be an autoimmune disease and is more common in women. Symptoms include degeneration of the soft tissue, typically on one side of the face.
| Condition | Characteristics |
|---|---|
| Bell palsy | Unilateral facial weakness and drooping; difficulty closing an eye; loss of furrows in the brow; most cases resolve spontaneously |
| Neurosarcoidosis | Bilateral or unilateral seventh cranial nerve palsy; other cranial nerve palsies can also be associated; most resolve spontaneously but may recur |
| Parry-Romberg syndrome | Unilateral facial atrophy; includes degeneration of the soft tissue on one side of the face; autoimmune reaction; more common in women |
| Ramsay Hunt syndrome | Unilateral peripheral facial palsy; herpes zoster infection of the external ear or tympanic membrane with involvement of facial or auditory nerves; tinnitus, vertigo, or deafness may occur |
