
Screening and Prevention
Skin cancer is the most common cancer in the United States.
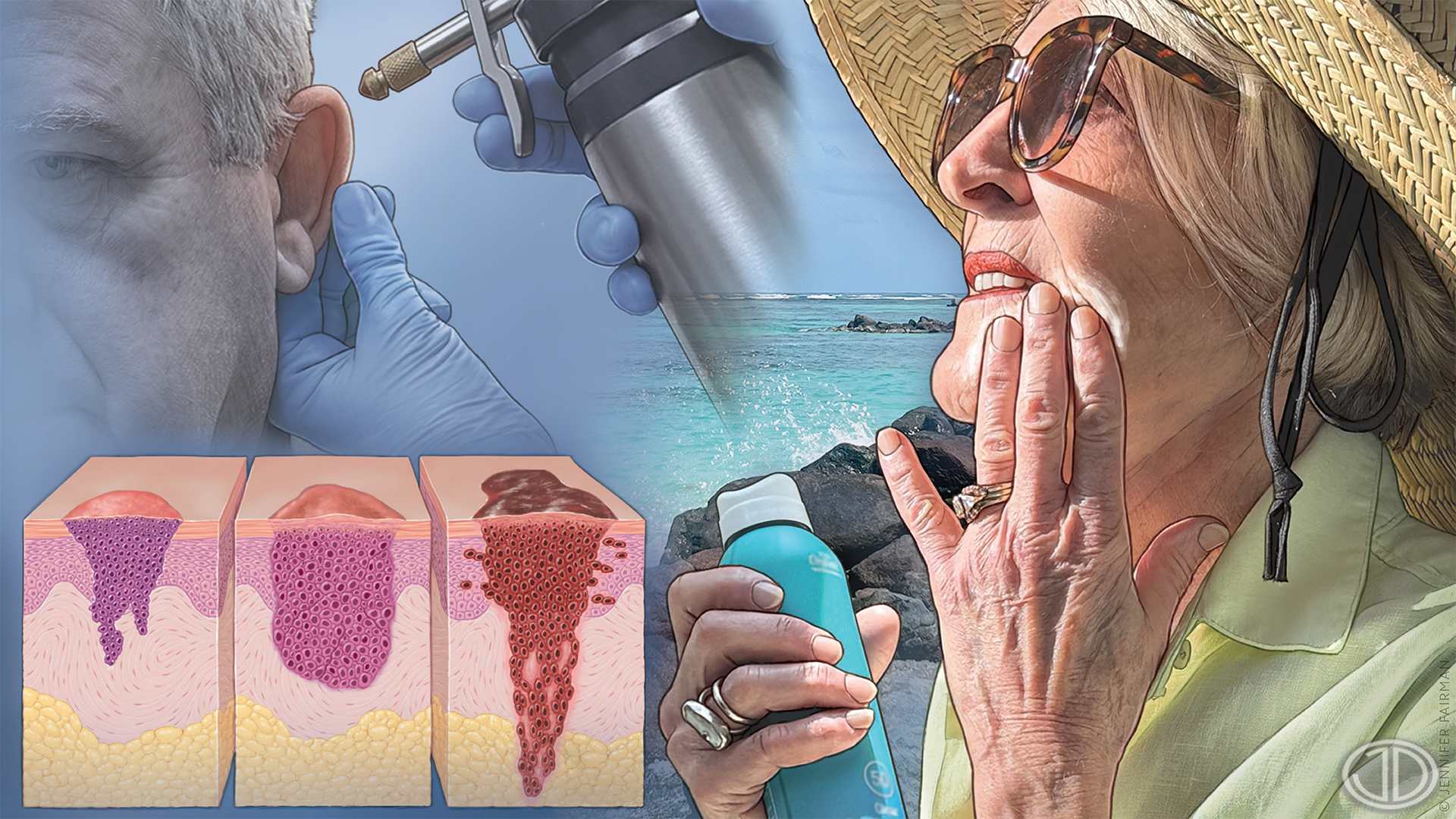
Diagnosis
Family physicians play a critical role in early detection of skin cancers. Although visual inspection is the initial step, dermoscopy significantly improves diagnostic accuracy, particularly for melanoma and basal cell carcinoma. Advanced imaging technologies such as reflectance confocal microscopy, optical coherence tomography, and high-frequency ultrasonography may further enhance accuracy and reduce unnecessary procedures. However, these technologies are primarily used in academic or specialty dermatology settings. Biopsy is required for definitive diagnosis. For nonmelanoma skin cancers, no single biopsy technique has demonstrated superiority. A shave, punch, incisional, or excisional technique should be selected based on lesion characteristics, patient factors, and clinical judgment. For melanoma, excisional biopsy with margins of 1 to 3 mm and full-thickness removal is preferred. Saucerization (deep shave removal of the entire clinical lesion to the mid-dermis or deeper) may be acceptable if it allows accurate assessment of Breslow depth. Basal cell carcinoma subtypes include nodular, superficial, morpheaform (sclerosing), and infiltrative. Cutaneous squamous cell carcinoma is classified as in situ or invasive. The clinical subtypes of melanoma include superficial spreading, nodular, lentigo maligna melanoma, amelanotic, and acral lentiginous. If biopsy is not feasible because of lesion location or clinical suspicion persists despite benign histology, prompt dermatology referral is warranted.
Management of Actinic Keratoses and Keratinocyte Carcinomas
Actinic keratoses are precancerous skin lesions that are treated to prevent progression to cutaneous squamous cell carcinoma. Keratinocyte carcinomas include basal cell carcinoma and cutaneous squamous cell carcinoma. Cryosurgery is preferred to treat a single or limited number of actinic keratosis lesions, whereas field-directed therapies, such as topical fluorouracil, topical imiquimod, photodynamic therapy, topical tirbanibulin, and off-label topical fluorouracil plus calcipotriene, are preferred treatments for multiple lesions or significant field cancerization. For basal cell carcinoma, low-risk lesions may be treated with standard surgical excision, electrodesiccation and curettage, or topical agents for superficial subtypes. Basal cell carcinoma that is high risk or in cosmetically or functionally sensitive areas warrant Mohs surgery or similar techniques that provide complete margin assessment. Squamous cell carcinoma in situ can be managed with topical therapies, photodynamic therapy, electrodesiccation
and curettage, or Mohs surgery for high-risk sites. Invasive cutaneous squamous cell carcinoma should be treated surgically, typically with 4- to 6-mm margins for low-risk tumors and Mohs surgery for tumors that are high-risk or located in cosmetically or functionally sensitive areas. Radiation is an alternative for patients who are not candidates for surgery. Systemic hedgehog pathway inhibitors are approved for locally advanced or metastatic basal cell carcinoma in patients who are not candidates for surgery or radiation therapy, although adverse effects often limit tolerance. Checkpoint inhibitor immunotherapy can be used in certain advanced cases of basal cell or cutaneous squamous cell carcinoma.
Management of Cutaneous Melanoma
Melanoma is the fifth most common cancer in the United States and one of the deadliest. Tumor depth (Breslow depth) is the most important prognostic factor. Wide local excision is used to manage melanoma stage 0 (in situ) with 0.5- to 1-cm margins, as well as stage IA with 1-cm margins. For lentigo maligna (melanoma in situ), surgical margins wider than 0.5 cm are often necessary to achieve histologically negative margins, and comprehensive margin assessment techniques (Mohs surgery or staged excision) are associated with lower recurrence rates. Localized melanoma with a Breslow depth of less than 0.8 mm and without ulceration has an excellent prognosis and low risk for metastasis; standard treatment is wide local excision with 1-cm margins. Referral is required for melanoma stage IB or higher for discussion of sentinel lymph node biopsy and consideration of adjuvant therapies. Advances in sequencing have enabled tailored therapies for metastatic melanoma based on variations in somatic genes. Immunotherapy has improved survival in those with advanced melanoma. Genetic counseling should be considered for patients with a personal or family history of melanoma or certain other cancers (notably pancreatic cancer, uveal melanoma, mesothelioma, or astrocytoma). After a melanoma diagnosis, patients should undergo full skin examinations at least annually for surveillance.
Past Editions
#563 | Obesity Management
See full issue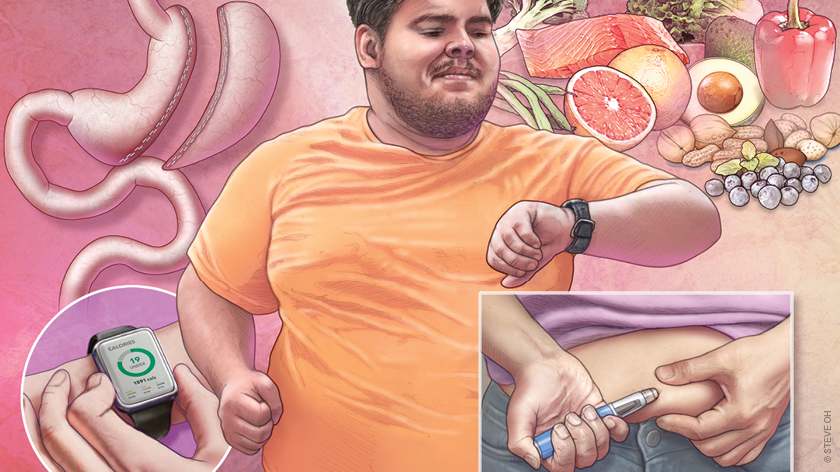
Evaluation
Obesity is a multifactorial, chronic condition that substantially affects individual and public health, reduces life expectancy, and increases the risk for a wide range of comorbid conditions (eg, cardiovascular disease, hypertension, depression, liver disease, type 2 diabetes…
Lifestyle Interventions
Obesity management in primary care should begin with lifestyle interventions for patients ready to engage in behavior change. Using the 5As counseling model (assess, advise, agree, assist, arrange) in a patient-centered, nonjudgmental manner enhances motivation and adherence…
Pharmacotherapy
Anti-obesity drugs should be offered as initial treatment of overweight and obesity for adults with weight-related comorbidities and for those at high risk of complications, and as a component of first-line treatment for patients with obesity and overweight without…
Surgical Interventions
Metabolic and bariatric surgery (MBS) is surgery on the gastrointestinal tract aimed at weight loss and resolution of metabolic disease. These surgeries can result in remission of diabetes, hypertension, and sleep apnea in many patients, and can prolong life expectancy by 5 to…

