
Am Fam Physician. 2024;110(2):130A-130B
Author disclosure: No relevant financial relationships.
Family medicine is financially undervalued compared with other medical specialties, and reimbursement fails to recognize the valuable longitudinal care provided to patients. According to one estimate, a primary care physician earns approximately $80,000 less than a subspecialist peer in Medicare reimbursement over a one-year period.1 This gap persists despite primary care physicians addressing higher numbers of medical concerns during office visits. To address continuity, the Centers for Medicare and Medicaid Services created the G2211 code in 2019 to compensate for the “visit complexity inherent to evaluation and management associated with medical care services.”2 The G2211 code was implemented in January 2024.
The Centers for Medicare and Medicaid Services has made previous changes to increase reimbursement and reduce documentation burden, such as the 2021 Evaluation and Management (E/M) coding rule changes, which led to a 10% increase in Medicare revenue.3 The G2211 code may be used in combination with E/M codes.
Although the G2211 code offers increased payment for primary care visits, it cannot be used with a 25 modifier. This modifier is commonly used to account for additional work during a primary care visit, including procedures, vaccinations, and additional diagnoses addressed. Unlike the G2211 code, which adds $17.29 to each continuity visit, the 25 modifier value differs based on the E/M level and the procedure attached. For example, a 25 modifier for the lowest-level E/M code would result in a $45 reimbursement for an established patient visit, whereas the highest-level E/M code would result in a $148 reimbursement.
To better understand the impact of the G2211 code on revenue, the authors used the 2018 Medicare Part B carrier data to define a cohort of 2.49 million beneficiaries with select chronic conditions across 9,500 sampled primary care physicians and collected the G2211-eligible E/M codes (99202-99205; 99212-99215; n = 2,162,000 claims).4 Of those, 583,000 claims with a 25 modifier code attached were identified. A 25 modifier “premium” per visit was calculated using an average of 2024 E/M fee schedule rates weighted by the frequencies of occurrence of these E/M codes. The weighted average of each 25 modifier was $117. The authors calculated the revenue stream using G2211 adoption for new and established E/M claims (n = 1,579,000) that previously did not have an associated 25 modifier. The potential net monetary gain of using the G2211 modifier for the 583,000 claims associated with a 25 modifier was also calculated.
If used for all eligible visits, the G2211 code results in an increased total reimbursement of $25.3 million annually, or $2,667 on average per physician in the study sample. If the G2211 code were allowed to be used in addition to the 25 modifier, an additional $9.4 million could potentially be generated (Figure 1). If used in only 50% of visits in conjunction with a 25 modifier, approximately $5 million would be added to primary care revenue.
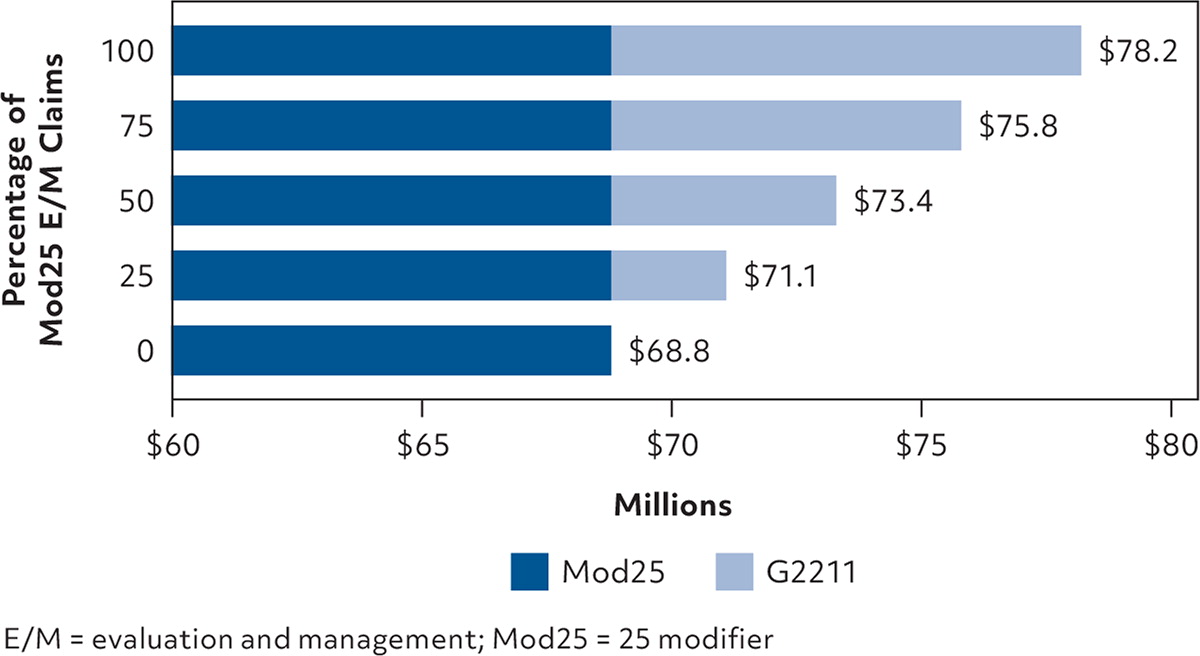
This model shows that primary care physicians stand to gain modestly increased reimbursement from adding the G2211 code on E/M visits when a 25 modifier is not used. However, the G2211 code should not be used instead of the 25 modifier. If the G2211 code were eligible to be used in addition to 25 modifiers, another $9.4 million, or $990 per physician, could be generated. Physicians should consider two takeaways: incorporate the G2211 code into daily billing practice, and advocate for the G2211 code to be used in conjunction with the 25 modifier.
